Acute Effect of a Flywheel Exercise on Cardiac, Hemodynamic, Autonomic, and Neuromuscular Responses
- 1. Markes Studio, Brazil
- 2. Virya Moviment, Brazil
- 3. Sport Club Corinthians Paulista, Brazil
- 4. Campinas University, Brazil
- 5. Nucleus of High Performance in Sport?NAR, Brazil
- 6. Reference Center in Sport Science, Social Service of Industry, Brazil
ABSTRACT
Flywheel (FW), apparatus is a non-gravity-dependent exercise system that has been proposed to increase eccentric workload and skeletal muscle strength. The acute effect of FW exercise on cardiac, hemodynamic, autonomic, and neuromuscular responses remains scarce. The present study aimed investigate the heart rate (HR), blood pressure (BP), HR variability (HRV), and vertical jump performance (VJ), following a FW exercise. The effort consisted of 4 sets x 12 repetitions on the half squat exercise executed with 3 flywheel rotations and 1-min of intervals between sets. HR was assessed during all experimental session. BP and VJ were assessed pre and immediately 5-, 20-, and 35-min post-exercise. HRV was evaluated by root mean square of the successive differences (RMSSD), at rest, 20-, and 35-min post-exercise. The ANOVA one way was applied followed by Bonferroni´s post hoc test if necessary. The FW moderately improved the cardiac and hemodynamic stress with a concomitant reduction on HRV. The VJ performance was not significantly affected at 5-min post FW exercise, but was impaired at 20-min and remained reduced until 35-min post-exercises. In conclusion, the FW induced a moderate stress in cardiac and hemodynamic responses followed by a decrease in the HRV. In addition, the FW impaired the jumping ability at 20- and 35-min of passive recovery. These findings are important to better comprehend the physiological responses of a FW exercise.
KEYWORDS
Strength training, Eccentric actions, Heart rate variability, Cardiovascular stress.
CITATION
Chediac CM, Zanotto PB, Kobal R, Cal Abad CC (2022) Acute Effect of a Flywheel Exercise on Cardiac, Hemodynamic, Autonomic, and Neuromuscular Responses. Ann Sports Med Res 9(1): 1185.
ABBREVIATIONS
SE: Strength Exercise; PEH: Post-Exercise Hypotension; PAP: Post Activation Potentiation; FW: Flywheel; HR: Heart Rate; BP: Blood Pressure; HRV: Heart Rate Variability; VJ: Vertical Jumping Ability; iRR: RR Intervals of Electrocardiogram Signals; RMSSD: Root Mean-Square Differences of Successive Normal; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; SJ: Squat Jump; CMJ: Countermovement Jump.
INTRODUCTION
Strength exercise (SE), has been recommended for several healthy institutions for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness [1,2]. However, some SE models promotes greater cardiac stress and reductions in post-exercise sympathovagal balance than traditional aerobic dynamic exercise such as walking, running, or cycling [3,4]. Thus, SE prescription requires caution since a lower vagal reactivation or a higher sympathetic hyperactivity (later heart rate recovery), observed post-exercise may be related with morbidity and all cause of mortality [5-7]. Hence, the SE may be carefully prescribed to promote neuromuscular adaptations and on the same way minimize possible cardiac and hemodynamic risks, especially in people with chronic diseases. In addition, SE can be prescribed with very distinct purposes such as to promote a cardiac protective effect of post-exercise hypotension (PEH), [8,9] or for an acute physical performance enhancement by means of a post activation potentiation (PAP), [10-12].
SE is commonly prescribed using traditional gravitydependent weight machines, free-weights, or the body weight. The effects of this type of SE on hemodynamic, autonomic, and neuromuscular responses have been extensively investigated [13-15]. However, the knowledge about physiological and neuromuscular responses of nontraditional strength training devices such as flywheel (FW), machines remains relatively scarce. Therefore, such responses remain to be stablished in order to practitioners to safely prescribe this exercise. FW consists of a non-gravitational and non-motorized device that offers resistance during coupled concentric and eccentric actions by utilizing the inertia of rotating flywheels [16]. Initially designed for space crew in orbit, it has been used for SE and has been considered a good tool for increasing eccentric actions. In addition, FW elicits early and robust neuromuscular adaptations such as muscle strength, power, and size than traditional SE [17- 20]. To date, the acute effect of FW on cardiac, hemodynamic, autonomic, and neuromuscular responses remains unknown.
Therefore, the present study aimed to investigate the response of heart rate (HR), blood pressure (BP), heart rate variability (HRV), and vertical jumping ability (VJ), following an acute FW exercise bout. We hypothesized that a classical FW exercise for lower limb would induce moderate to high hemodynamic and cardiac stress followed by a reduction on HRV, PEH and PAP.
MATERIALS AND METHODS
This cross-sectional study aimed to check the acute effect of a FW exercise bout on cardiac, hemodynamic, autonomic, and neuromuscular responses. The experimental session was composed of anthropometric (i.e.; body height and body weight measurements), 10-min of rest, 10-min of warm-up, a FW exercise bout, and, finally, 35-min of passive recovery. Before the experimental session, two familiarization sessions interspersed from 48- to 96-h were conducted. The experimental session occurred one week after the last familiarization session. The volunteers were oriented to maintain their routines concerning sleep and nourishment during the last 48-h before the experimental session. They were also oriented to avoid caffeine ingestion or anything substance that could to affect autonomic, hemodynamic or neuromuscular response two hours prior to the experimental session. The 10-min of rest condition occurred before the warm-up. During this phase, the participants remaining on a sitting position, quiet, open eyes, and free breathing. The 10-min of standardized general warm-up consisted of 5-min of a 6-km running followed by 5-min of lower limb dynamic and active stretching (30s for each muscle group). The specific warm-up was composed of 2 submaximal SJ, 2 submaximal CMJ (both interspersed with 10s of interval between the attempts and 30s between exercises), and 5 submaximal repetitions in FW apparatus. Five minutes after the warm up the measurements were started, and the FW exercise was performed. After the FW exercise bout, the participants remaining 35-min on passive recovery at the same condition than the rest (i.e; sitting position, quiet, open eyes, and free breathing). The schematic view of the experimental session is described in Figure 1.
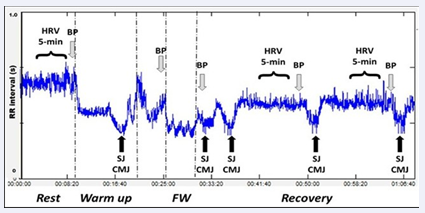
Figure 1 An example of a typical RR interval registration acquired during rest, warm up, flywheel exercise (FW), and recovery phase of overall
experimental session.
SUBJECTS
The volunteers were invited to compose the sample of the study and were submitted at a previous anamnesis. Subjects with orthopedic or cardiovascular injuries or diseases in the last six months before the study were considered ineligible to compose the sample. Were considered eligible only physically activity and healthy volunteers that do not use any ergogenic, supplement, and/or medicine that could to affect the responses of the main variables investigated in the study during 4 weeks before the beginning of the study. After receiving a thorough explanation of the possible risks and discomforts associated with the experimental procedures, they gave their written informed consent. All procedures were conducted according to the Helsinki Declaration. The study was approved by a local ethical committee. All participants were familiarized with measurements. The procedures were conducted in the morning from 09:00 to 12:00 a.m. or in the afternoon from 14:00 to 17:00 p.m. with optimal environmental conditions (i.e.; 20-25 ºC and relative humidity 60-75%). Overall, 13 health subjects (36.46 ± 6.69 years, 177.66 ± 3,93 cm 79.42 ± 8.69 kg) volunteered to participate in the study.
PROCEDURES
Heart rate and heart rate variability
Both HR and HRV were assessed using the RR intervals (iRR), obtained by a portable HR monitor (Polar® RS800cx, Kempele, Finland) at a sampling of 1,000 Hz, continuously during all experimental session [21, 22]. Data were automatically inspected to identify artifacts and ectopic beats (<3%), which were manually removed and replaced by interpolation of adjacent iRR. The iRR were downloaded via accompanying Polar software (Polar® ProTrainer, Kempele, Finland) and exported for later analysis of time domain measures of HRV by Kubios software [23]. The rest HR was assessed using the mean of the last 2-min during the rest condition. The HR of FW exercise was obtained using the mean of the HR measured during the FW bout. The HR during the recovery phase was assessed using the last 1-min of each 5-min. The root mean-square differences of successive normal (RMSSD), was assessed at rest, 20-, and 35-min after the FW exercise regarding the last minute of 5-min of higher iRR stability.
Blood pressure
The BP was obtained indirectly using an automatic oscillometric device (HEM-705CP; Omron Healthcare, Vernon Hill, IL, USA). Both systolic (SBP), and diastolic (DBP), blood pressure were registered at rest, after the warm up, after the FW exercise, at 20-, and 35-min post FW exercise.
Vertical jumping ability
The neuromuscular performance was evaluated by vertical jumping ability using the height jump of both squat (SJ) and countermovement (CMJ) jumps. The flight time was assessed by a standardized, valid and reproducible device by the flight time assessed by a contact plat (Elite Jump, São Paulo, Brazil) [24]. For SJ assessment, the participants started from an upright standing position with their hands on their hips. Subsequently, they were instructed to flex their knees and hold an optimal auto selected knee position. Finally, they were instructed to jump as high as possible without performing any countermovement before the execution of the jump. For CMJ, subjects started from the upright standing position with their hands on their hips. Next, they were instructed to flex their knees as quickly as possible and then jump as high as possible in the ensuing concentric phase. For all jumps, it was recommended that they leave the floor with knees and ankles extended and land in a similarly extended position. All sessions were supervised by an evaluator with 5-years’ experience. Two attempts for each vertical jump (i.e.; SJ and CMJ) were performed. Each attempt was interspersed with a 15-s of recovery period. The best height jump was considered for analysis.
Flywheel exercise bout
FW machine have rotating shafts and a belt. The belt was attached to the subject´s waist, cords run from the belt to the shaft. The cords were wrapped around the shaft and transfer the subject’s movement into kinetic energy which rotates the shaft. The Figure 2
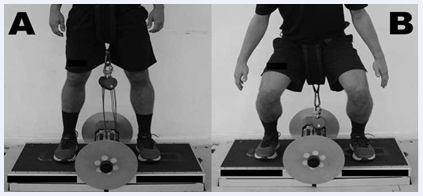
Figure 2 The half squat flywheel machine at knee extension (A = concentric action), and flexion (B = eccentric action).
illustrates the FW exercise.
The FW exercise bout was composed of 4 sets x 12 repetitions on the half squat exercise executed with 3 flywheel rotations and 1-min of intervals between sets as previous described. As previously described, FW exercise repetitions were performed with maximal effort, accelerating the wheel in the concentric action and upon completion, decelerating the wheel by means of an eccentric action. The volunteers were oriented to push with maximal effort through the entire concentric action, which ranged from 70º knee flexion to near full extension. At the end of the concentric action, the strap winds back due to inertial a force, which initiates the reversed eccentric action. During the first three eccentric actions, subjects were instructed to resist gently, and thereafter to apply other 12 maximal repetitions. The breaking force to stop the movement was about 70º knee flexion [25,18].
Statistical Analysis
Statistical Analysis The normality of the data was checked using the ShapiroWilk test. Data were described as mean and standard deviation. To test mean differences among conditions a one-way ANOVA for repeated measures was applied. The significant level adopted was 5% (p<0.05).
RESULTS AND DISCUSSION
The HR responses are shown in Figure 3.
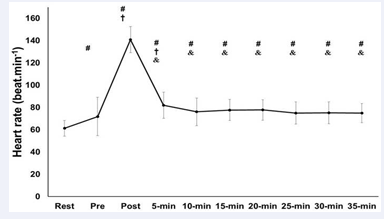
Figure 3 Heart rate response before, during flywheel (FW) exercise, and recovery periods. Abbreviations: # = different from rest; † = different from Pre; & = different from FW; p<0.05.
The FW exercise induces a moderate cardiovascular stress since the peak HR reaches ≈140 beats.min-1 (45% HR reserve). After the effort, the HR declines 40% at 5-min but remained significantly higher than warm up and rest conditions (p<0.05). Ten min after the bout the HR continued significantly higher than the rest (p<0.05) and do not return from the rest condition after 35-min of recovery.
The BP responses are in Figure 4.
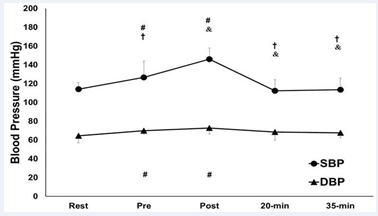
Figure 4 Blood pressure response before and after flywheel exercise.Abbreviations: SBP = systolic blood pressure; DBP = diastolic blood pressure; FW = flywheel exercise; # = different from Rest; † = different from Pre; & = different from Post; p<0.05.
The FW exercise improves SBP near to 140 mmHg increasing significantly in comparison to all other conditions (p0.05). The SBP of 15-, 20-, 30- and 35-min were significantly lower than at 5-min. Finally, the SBP at 20- and 35-min were significantly higher than at 10-min. Regarding the DBP, significant increasing was found at pre and immediately post in comparison to the rest condition (p<0.05).
The RMSSD is illustrated in Figure 5.
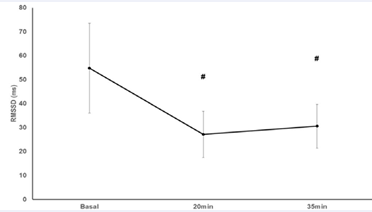
Figure 5 Heart Rate variability response before and after flywheel exercise. Abbreviations: # = different from Rest; p<0.05.
The HRV reduced significantly at 20- and remained significantly lower until 35-min post FW exercise in comparison to the rest condition (p<0.05).
The Figure 6
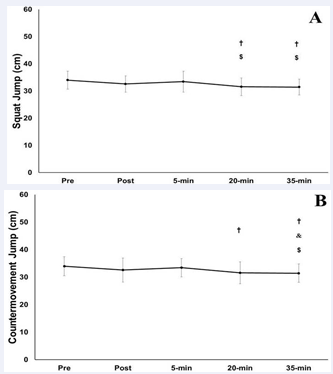
Figure 6 (A) Squat Jump and (B) Countermovement Jump responses before and after flywheel exercise. Abbreviations: † = different from Pre; & = different from Post; $ = different from 5-min; p<0.05.
reports the VJ responses. The SJ showed a significant reduction (p<0.05) at 20-min and 35-min in comparison to post and 5-min post exercise. Similarly, CMJ showed a significant reduction (p<0.05) at 20- and 35-min after the FW in comparison to rest. However, only 35-min showed a significant reduction in CMJ in comparison to immediately post and 5-min post exercise.
The purpose of the present study was to investigate the acute effect of a FW exercise session on cardiac, hemodynamic, autonomic, and neuromuscular responses. The main finding of this study was that FW induced a moderate cardiac and hemodynamic stress, a reduction in the HRV by 35-min postexercise whereas VJ performance was impaired from 20 to 35- min of recovery.
The cardiac and hemodynamic stress found in the present study is in accordance with previous studies that found increases in post-exercise HR and SBP after high-intensity lower limb exercises such as leg press and chair extension machine [14,26]. These responses were expected since FW consists of a dynamic exercise composed by a high-velocity concentric action followed by an overloaded eccentric activity that induces a high activation of the mechanoreceptors during the muscle contraction, and, consequently, requires a high activation of the central nervous system motor command [27]. In addition, FW exercise also increases arterial resistance, metabolites accumulation, and reduced venous return, stroke volume and cardiac output, which results in cardiovascular stress increasing [28].
The DAP showed a significant increase after the warm-up, and immediately post the FW exercise. However, it remained near of optimal values (i.e; <80mmHg) [29]. This response following strength exercise is controversy because some studies described reductions in DBP [30,8] whereas others found no changes [31-33], and others, equally to the present study, found an increasing [34-36]. Collectively, the discrepancies found in cardiac and hemodynamic responses among different studies may be explained due to several confounding factors such as participant status (i.e.; healthy vs. unhealthy, or sedentary vs. physically active vs. athlete), strength exercise type (load, intensity, volume), and interactions between several mechanisms of post-exercise adjustment in the BP and blood flow (i.e.; plasma volume and cardiac output) [37,38]. Nevertheless, because no direct physiological mechanisms were measured in the present study, future research using FW exercises are required to better elucidate how FW exercises could affect each before mentioned physiological variable.
FW did not induce post exercise hypotension (PEH). The absence of PEH in the present study may be justified because a recent met analytical study suggests that PEH is more accentuated in aerobic exercises such as jogging and in moderate to long sessions that includes a higher number of resistance exercises [39]. Indeed, PEH seems to be more pronounced in strength exercises performed for both upper and lower limbs, with higher set numbers (≥5), 8-10 repetitions, and at 70% of maximal strength [40,41]. Therefore, regarding that the present study was conducted using a FW exercise bout characterized by a high velocity concentric action followed by an eccentric overload in healthy subjects, it is reasonable to assume that this type of exercise prescription (i.e., 4 sets x 12 repetitions), was not capable to induce PEH. Perhaps a FW exercise performed with a higher volume, and lower inter-set recovery time could induce to a different cardiac and hemodynamic stress response. The influence of eccentric muscle action in hemodynamic response remains unknown both in traditional strength and in FW exercises. Future studies are necessary to better elucidate the role of this specific muscle action on hemodynamic responses.
The absence of PAP in the present study contrary previous reports and suggest that other exercises such as dynamic and ballistic stretching, plyometric drop jump, whole body vibration, and complex training including high load exercises followed by explosive actions seemed to induce PAP better than FW exercises [42-44]. However, is important to note that even without PAP, the FW also not impaired VJ performance after a short recovery (<5- min). This is an important finding since acute eccentric overloads could prejudice skeletal muscle structure and neuromuscular function, and impair neuromuscular performance [45]. Collectively, our result suggests that the FW exercise applied in the present study seemed to be not enough to play neither positive nor negative influence in VJ performance. The better FW exercise capable to induce PAP remains unknown so that future studies are required to investigate if other FW exercise design could induce PAP.
uld induce PAP. The VJ impairment may be explained by acute neuromuscular fatigue or muscle damage induced by eccentric workload [46-48] Another reason for VJ decreasing after 20-min is, probably, the cool down since the subjects remaining in rest condition more than 15-min after the FW exercise bout. Although the body temperature was not measured and this argue is speculative, the cool down response is strongly supported with a recent met analytical study suggesting optimal warmup duration near to 10- 15-min combined, a passive rest between 2 and 10 min before the main performance, and a re-warm-up with short-term sprints and jumps for transitions longer than 15 min [49].
There are some limitations to the current study. First one was the small sample size which may reduce the ability to expand the results for other population. Second, is the absence of a control group both comparisons between FW and others SE. Finally, the short time of attendance (i.e.; 35-min). Future studies to investigate the long-term effect of FW in a large sample size including health and disease people compared with other SE are required.
CONCLUSION
In conclusion, the FW increases the cardiac, hemodynamic, and autonomic stress, but do not affect vertical jumping ability after a short period (5-min), of recovery. This information may be considered to prescribe FW exercise training in health adults. The mechanisms that can justify these physiological and neuromuscular responses may be clarified in future studies.







































































































































