A Case of First Manifestation of Systemic Sclerosis with Peripheral Angiopathy
- 1. Mariahilf Health Center, Austria
Abstract
A 64 y/o female patient was referred to our clinic for a vascular check because of blue left index finger since three weeks. She had been experiencing the Raynaud-phenomenon on her fingers for thirty years, but it was not limiting her daily routine; a single workup many years earlier reportedly did not reveal a cause. Otherwise, she was treated for arterial hypertension, hyperlipidaemia and depression. Her medication consisted of a statin, blood pressure lowering medication and antidepressants. She was a non-smoker and had no allergies
Keywords
• Raynaud’s, Blue finger, Peripheral angiopathy,
Scleroderma
Citation
Luka G (2021) A Case of First Manifestation of Systemic Sclerosis with Peripheral Angiopathy. Ann Vasc Med Res 8(3): 1135.
CLINICAL PRESENTATION
Clinically the patient presented with a blue left index finger with a markedly prolonged capillary refill time, and there was a small skin defect at the tip of the finger. Other fingers were clinically unapparent. The right radial pulse was palpable, the ulnar was not; on the right hand both pulses were palpable.
In the optical oscillography, there were no oscillations on the left index finger, strongly reduced oscillations on the left middle finger, and somewhat reduced oscillations on all other fingers of both hands.
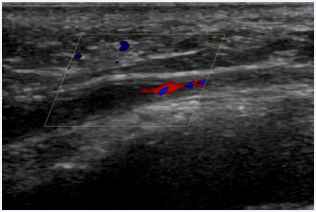
Figure 1 Occlusion of the distal left ulnar artery.
On ultrasound scan, the perfusion of the left radial and ulnar artery (Figure 1) was normal up to the wrist, but distal the wrist joint there was a complete occlusion of the ulnar artery.
In capillary microscopy (Figure 2) enlarged capillaries (mega capillaries) and avascular fields were detected, a picture typical of scleroderma existing for a longer time but being an active disease.
Pathological laboratory findings were sedimentation rate 41mm/1h, ANA (anti-nuclear antibodies) 1: 10240, highly elevated anticentromere antibodies anti-CENP-B (+++), and mildly elevated Ro-52-antibodies (+).
Magnetic resonance -angiography showed arterial obstruction of carpal arteries, the thin ulnar artery ended in the hypothenar.
In addition, the ultrasound scan revealed carotid plaques and plaques in abdominal aorta without a high-grade stenosis or an aneurysm.
X-ray of the hands revealed arthrosis but no signs of inflammatory destructive process in the bone.
The pulmonary function was normal.
An echocardiography scan showed a lightly dilated left atrium, a concentric left ventricular hypertrophy, a middle grade aortic stenosis, a diastolic dysfunction I, and a low-grade tricuspid valve insufficiency. The echocardiographic findings were interpreted as related to arterial hypertension and not scleroderma.
The consulted rheumatologist diagnosed systemic sclerosis sine scleroderma.

Figure 2: Capillary microscopy in scleroderma.
We prescribed 100mg aspirin o/d in addition to her medication and gave her iloprost (10µg in the saline solution) infusions o/d for 20 days. In addition, the patient received subcutaneous enoxaparin 6000IU o/d for ten days because we suspected a sudden aggravation of pre-existing vascular abnormalities, which might be thrombotic in nature. The addition of the low-molecular heparin did not however improve either symptoms or the curve on optic oscillography and therefore we discontinued this medication.
The colour of the left index finger changed to near normal within a month, but pain persisted for a longer period. Three months later the patient was asymptomatic.
CONCLUSION
We present a patient with a peripheral vascular angiopathy as complication of scleroderma. Peripheral vascular changes, primarily of ulnar arteries, are frequent in patients with digital ulcers [1]. In our case the symptom of the the peripheral ischemia was a blue finger. Retrospectively, the long-time pre-existing Raynaud-syndrome might have been caused by scleroderma, but because it had been checked only once many years ago, it is not possible to draw conclusions. In any case, it seems safe to say that even a primary (or probable primary) Raynaud-syndrome should be reexamined from time to time for a possible cause of the secondary Raynaud-Syndrome.







































































































































{kind=link}