Primary Cutaneous Nocardiosis
- 1. Division of Infectious Diseases, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, and Chang Gung University College of Medicine, Kaohsiung, Taiwan
Citation
Chien-Hsiang T, Ing-Kit L (2021) Primary Cutaneous Nocardiosis. JSM Clin Case Rep 9(3): 1194
CLINICAL IMAGE
An otherwise healthy 80-year-old female was a housewife but had habit of handling ginger. She presented to the hospital with pain, erythema, swelling, and pustules over right lower leg for 2 days (Figure A).
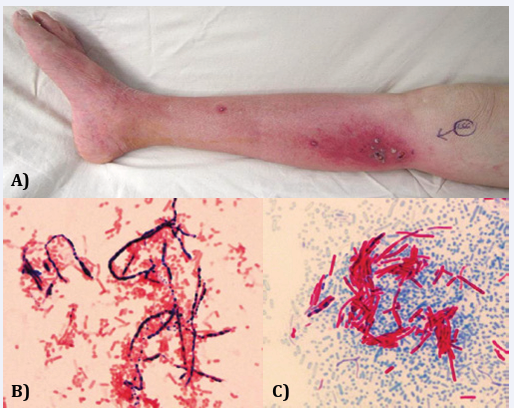
Figure 1 Right lower leg.
The symptoms progressed rapidly. The physical examination showed that her temperature was 38.0?, and her blood pressure was 144/92 mmHg. The right lower leg was swollen, with some pustules over it. Right lower extremity was warm, but the patient was very painful when examination. Computed tomography of lower extremity showed soft tissue inflammatory change with subcutaneous fluid accumulation over right lower leg. Emergent fasciotomy was performed. Staining of the pus collected during surgery showed grampositive branching rods (Figure B). It was also positive for modified acid-fast stain, using 1% sulfuric acid as a decolorizer (Figure C). Cultures grew Nocardia species. Nocardia species are environmental saprophytes and can be found in soil or organic matter. Human are infected by direct inoculation of the skin or by inhalation. Although immunocompromise is a risk factor for nocardiosis, primary cutaneous nocardiosis can develop in immunocompetent hosts, as our patient [1]. The patient received debridement few days later and was treated with trimethoprimsulfamethoxazole for 3 weeks. The patient was doing well and continued to take oral trimethoprim-sulfamethoxazole for 3 months after discharge.







































































































































{kind=link}