Marginal Microleakage of Bulkfill Restorations Submitted to Mechanical and Thermal Aging: An In vitro Study
- 1. Department of Restorative Dentistry, University of Campinas. Brazil
- 2. Department of Restorative Dentistry, Instituto Nacional de Ensino Superior e Pós-Graduação Padre Gervásio. Brazil
Abstract
Background: Bulk-fill composites emerged to enable deep restorations in single placing. Although they seem promising, their aging must be investigated.
Purpose: To evaluate the marginal microleakage of restorations made with bulk-fill and conventional composites, submitted or not to mechanical and thermal aging.
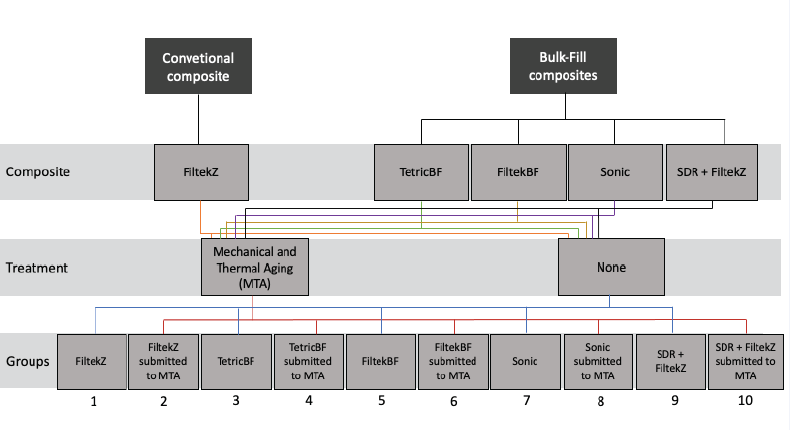
Material and Methods: Five millimetres deep Class II cavities were restored with bulk-fill (Tetric N-Ceram Bulk-fill - TetricBF, Filtek Bulk-fill Posterior Restorative – FiltekBF, SonicFill - Sonic) or conventional composites (Filtek Z350 XT - FiltekZ, and Surefil SDR Flow as base + Filtek Z350 XT – SDR + FiltekZ). Mechanical and thermal aging were performed following the restoration. Teeth were allocated in 10 groups (n = 10) based on type of composite and performance or not of mechanical and thermal aging. Dental blocks of all group were immersed in 2% methylene blue solution. Marginal microleakage was analyzed through Spectrophotometry. Data were submitted to two-way ANOVA and post-hoc Tukey’s test.
Results: FiltekZ presented highest microleakage, while TetricBF and FiltekBF showed lowest microleakage, regardless of being aged or not. Aged TetricBF and Sonic showed higher results of microleakage than not aged TetricBF and Sonic.
Conclusions: Bulk-fill composites restorations presented lower marginal microleakage than conventional composite restorations. However, bulk-fill composites were more prone to the effects of aging than conventional composite.
Citation
Pereira R, de Lima Marques JF, de Campos Serain I, Silva BG, Nunes Leite Lima DA, et al. (2022) Marginal Microleakage of Bulk-fill Restorations Submitted to Mechanical and Thermal Aging: An In vitro Study. JSM Dent 10(1): 1138.
Keywords
Bulk-fill composites, Dental Leakage, Dental Restoration, Permanent, Stress, Mechanical
ABBREVIATIONS
AFM: addition-fragmentation monomers; AUDMA: aromatic urethane dimethacrylate; Bis-EMA: ethoxylated bisphenol-A dimethacrylate; Bis-GMA: bisphenol-A diglycidyl ether dimethacrylate; EBPDMA: ethoxylated bisphenol-A dimethacrylate; PEGDMA: polyethylene glycol dimethacrylate; TEGDMA: triethyleneglycol dimethacrylate; UDMA: urethane dimethacrylate. Data were provided by manufacturers.
INTRODUCTION
Resin-based composite is the main material of choice for direct dental restorations, and has been extensively employed for decades, despite its limitations. During polymerization, all composites shrink to the limelight, leading to stress concentration and consequently, cohesive and adhesive failures [1]. Clinically, such failures may generate marginal gaps, postoperative sensitivity, marginal microleakage and secondary
caries [2]. Impairments related to composite polymerization can be minimized through incremental placement technique [1,3]. The monomers conversion degree is higher and the stress due to the polymerization shrinkage may be better controlled through decrease of material volume and C-factor [4]. However, considering that each increment should be light activated for at least 20 seconds, incremental technique is time consuming [5].
Bulk-fill composites emerged to reduce polymerization shrinkage inherent to resin-based composites, improve speed and efficiency of restoration procedure. Manufacturers claim that polymerization of bulk-fill composites is possible in 4-6 mm single increments [6]. Besides reducing polymerization shrinkage and saving time, the restorative technique allows less chance for technical errors, such as void incorporation and contamination between layers [7,8].
Among strategies in the formulation of bulk-fill composites are the use of more responsive light activators, which are able to absorb irradiance energy in deep layers; decrease on particles number, rendering the composite more translucent and favouring the passage of light; use of specific monomers for stress relief; and addition of new types of fillers, such as prepolymerized particles and fiberglass rod segments [8,9].
Although all strategies seem promising for achieving success in fast and efficient restorative procedures, there is no consensus in literature as to the actual advantage of using bulk-fill composites. Furthermore, once the advent of bulk-fill composites is relatively recent, there are few studies of their long-term performance [10]. While randomized clinical reports with a longer follow-up period are not published, studies that reliably simulate clinical scenarios of bulk-fill restorations aging are necessary.
For this reason, this study aimed to evaluate quantitatively the marginal microleakage of bulk-fill and conventional composite restorations, submitted or not to mechanical and thermal aging. The null hypothesis tested was that there would be no difference on microleakage of conventional and bulk-fill composites, independent of being aged or not.
MATERIALS AND METHODS
Teeth preparation
A hundred freshly extracted healthy bovine incisors were collected and randomly selected. The teeth outer surfaces were cleaned by root scaling and fluoride-free prophy paste application (Pert-X - SS White, Rio de Janeiro, RJ, Brazil).
In order to make the experiment closer to a real clinical situation and considering the teeth would be submitted to mechanical cycling, periodontal ligament, as well as alveolar bone were simulated, as previously described by Soares and colleagues (2005) [11]. Initially, each root tooth was immersed in melted utility wax up to 2 mm below cementoenamel junction, allowing the root to be covered by approximately 0.2 mm wax layer (Figure 1A).
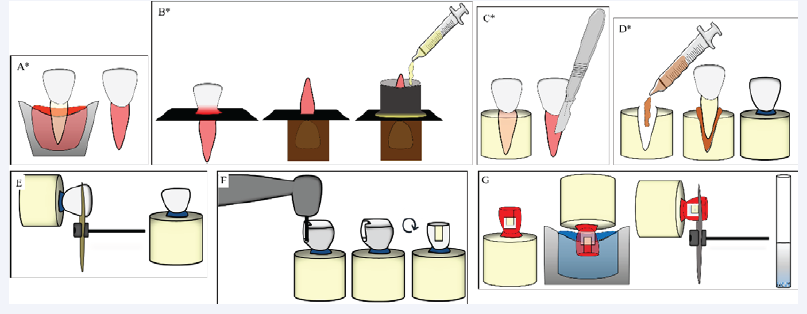
Secondly, the wax-covered root was included in polystyrene resin (V.I. Fiberglass, Guarulhos, SP, Brazil). A centrally perforated radiographic film (Contrast Speed E - Nova DFL, Rio de Janeiro, RJ, Brazil) was used to stabilize the tooth. The set was placed over a perforated wood plate, so as the coronary portion and 2mm of cementoenamel junction remained inside the perforation, while the wax-covered root was outside, separated by the film. A pipe of PVC (Tigre S.A. - Tubos e Conexões, Rio Claro, SP, Brazil) was then fixed around the root, on the radiographic film, with sticky wax. Polystyrene resin was poured into the pipe (Figure 1B). After polymerization, the pipe and radiographic film were removed, and simulated alveolar bone made of polystyrene resin was ready.
Lastly, to simulate periodontal ligament, the tooth was removed from “alveolar bone” using a #150 dental-surgical extracting forceps (Millennium, GOLGRAN, São Caetano do Sul, SP, Brazil). The remaining wax was taken off from the root tooth and “alveolar bone” with a scalpel blade, leaving a space of approximately 0.2 mm between the root and the “alveolar bone” (Figure 1C). Due to the similarity already described of
elastomeric materials used in impression procedures to the mechanical response of a soft tissue under external stress [11], a polyether-based impression compound (Impregum Soft - 3M Oral Care, St. Paul, MN, USA) was used to simulate the periodontal ligament. The material was manipulated according to the manufacturer instructions and inserted into the space created inside the “alveolar bone”. The tooth was reintroduced under digital pressure and the excesses of the impression material were removed using a scalpel blade (Figure 1D).
Finalizing the periodontal ligament simulation and inclusion of all teeth in “alveolar bone”, a cut was made 7 mm above the proximal cementoenamel junction of the teeth using a doublesided diamond disc (KG Sorensen, Barueri, SP, Brazil), thus obtaining a wide incisal surface (Figure 1E). The exposed surface was then polished with 600-grit silicon carbide abrasive paper (Norton, Guarulhos, SP, Brazil) fixed to a polishing machine (Aropol VV-PUD - Arotec, Cotia, SP, Brazil) until achievement of a flat dentin surface.
A custom-made apparatus was used for standardization of class II cavities of 5mm height, 4 mm wide and 1.5 mm deep. Preparation was made using #3146 carbide burs (KG Sorensen) at high-speed, under constant water cooling.
Restorative procedure
First, a circumferential straight metal matrix was positioned around the tooth with the aid of a Tofflemire retainer (Golgran, São Caetano do Sul, SP, Brazil). Enamel and dentin were etched with 35% phosphoric acid (Ultra-Echt, Ultradent Products Inc., South Jordan, UT, USA) for 30 and 15 seconds, respectively, followed by abundant rinsing and gentle drying with a cotton ball. Then, two coats of a commonly used adhesive system on clinical practice (Adper Single Bond 2, 3M Oral Care, St. Paul, MN, USA) were applied with light scrubbing motion for 15 seconds, following the manufacturer instructions. After the last application, surfaces were air dried for 5 seconds and light-cured by polywave light emitting diode curing unit (VALO, Ultradent Products Inc., South Jordan, UT, USA) in Standard mode: 1000 mW/cm², for 10 seconds. Restorative procedure was performed according to groups/composite resin: GROUPS 1 and 2: Filtek Z350 XT (3M Oral Care, St. Paul, MN, USA) – FiltekZ; GROUPS 3 and 4: Tetric N-Ceram Bulk-fill (Ivoclar Vivadent, AG, Schaan, Liechtenstein) – TetricBF; GROUPS 5 and 6: Filtek Bulk-fill Posterior Restorative (3M Oral Care, St. Paul, MN, USA) – FiltekBF; GROUPS 7 and 8: SonicFill (Kerr Co, Orange, CA, USA) – Sonic; GROUPS 9 and 10: Surefil SDR Flow (DENTSPLY Caulk, Milford, USA) + Filtek Z350 XT – SDR + FiltekZ (Figure 2).
Composites of groups 3 to 8 were placed in single increment. Sonic was inserted with proper sonic-activation condensing device. Composite of groups 1 and 2 was placed in two increments of 2mm and 1 increment of 1mm. In groups 9 and 10, 4mm of SDR was placed as base, followed by 1mm of FiltekZ (Figure 1F). Composites increments were light-cured (VALO) in Standard mode (1000 mW/cm²) for 20 seconds. Finishing and polishing of restorations surfaces were performed with sequential flexible discs with aluminum oxide coating (Medium, fine and superfine grades, Sof-Lex Finishing and Polishing System, 3M Oral Care, St. Paul, MN, USA). Each disc was applied for 30 seconds. The information of the composites tested in this study are presented in Table 1.
Mechanical and thermal aging
In order to simulate aging at oral cavity conditions, after restoration, finishing and polishing procedures, groups 2, 4, 6, 8 and 10 were submitted to 200.000 mechanical cycles under 86 N load at 2 Hz in a mechanical cycling equipment (ER-37000, ERIOS, São Paulo, SP, Brazil) [12]. Load was applied on the middle of restoration. Samples were then thermal cycled (MSCT-3e, ElQuip, São Carlos, SP, Brazil) 550 times at temperature ranging from 5 ± 1 ° C, 37 ± 1 ° C and 55 ± 1 ° C in three separated water chambers, for 30 seconds each one, at 15 seconds interval.
Marginal microleakage test
Firstly, the area to be infiltrated, corresponding to cervical tooth-restoration interface, was protect with a strip of adhesive masking tape (6 x 4 mm) (Adelbras, Vinhedo, SP, Brazil). Then, two layers of nail polish (Impala, Guarulhos, SP, Brazil) were applied over the entire sample. After, the masking tape was removed, uncovering the cervical tooth-restoration interface, and samples were completely immersed in 2% methylene blue dye solution (Merck, Darmstadt, Germany) for 2 hours [13].
Samples were taken from the solution, rinsed under running water and dried. The nail polish was removed with a periodontal curette (Millennium, GOLGRAN, São Caetano do Sul, SP, Brazil) and restoration’s surface was light abraded with 30 seconds application of aluminum oxide flexible disc (Fine grade, Sof- Lex Finishing and Polishing System, 3M Oral Care, St. Paul, MN, USA) in order to remove any deposited dye. The cervical toothrestoration interface was block-shaped sectioned with a doublesided diamond disc. Blocks were then taken to a hard tissue grinder (MA-475, Marconi Equipamentos Ltda., Piracicaba, SP, Brazil) until obtaining a tooth/restoration-based powder. The blocks were weighted before and after being grinded to confirm no differences between initial and final masses.
| Material brand name (abbreviation) |
Manufacturer | Matrix composition | Filler type | Filler loading (weight%/ volume%) |
Shade |
| Filtek Z350 XT (FiltekZ) | 3M Oral Care (St. Paul, MN, USA) |
Bis-GMA, UDMA, TEGDMA, PEGDMA, Bis-EMA |
Silica, zirconia, aggregated zirconia/silica filler |
78.5/63.3 | A2E |
| Tetric N-Ceram Bulk Fill (TetricBF) |
Ivoclar Vivadent AG. (Schaan, Liechtenstein) |
Bis-GMA, Bis-EMA, UDMA |
Barium aluminium silicate glass, “isofiller” (cured dimethacrylates, glass filler and ytterbium fluoride), ytterbium fluoride, spherical mixed oxide |
76-77/61 | IVA – Corresponding to A2 or A3 |
| Filtek Bulk Fill Posterior Restorative (FiltekBF) |
3M Oral Care (St. Paul, MN, USA) |
AUDMA, AFM, UDMA, 1,12-dodecane-DMA |
Silica, zirconia, aggregated zirconia/silica filler, ytterbium trifluoride |
76.5/58.4 | A2 |
| SonicFill (Sonic) | Kerr Co. (Orange, CA, USA) |
Bis-GMA, TEGDMA, EBPDMA |
Silica, silicon dioxide, barium glass, oxides |
83.5/66 | A2 |
| SureFil SDR Flow (SDR) | DENTSPLY Caulk (Milford, USA) |
Modified UDMA, EBPADMA, TEGDMA |
Barium-alumino-fluoroborosilicate glass, strontium alumino-fluoro-silicate glass |
68/45 | A2 |
After grinding, the powder obtained from each sample was immersed separately in glass centrifuge tubes containing 4 ml of absolute ethanol (Merck, Darmstadt, Germany) for 24 hours in order to dissolve the dye that leaked through tooth-restoration interface (Figure 1G). The solutions were centrifuged at 3000 rpm for 3 minutes (Centrifuge IC 15NA, TOMY Digital Biology, Tokyo, Japan), so that powder and any impurities were decanted.
| Composite Resins | Mechanical and Thermal Aging | |
| No | Yes | |
| FiltekZ | 250,9 (88,9) aA | 204,0 (41,4) aA |
| TetricBF | 16,75 (5,6) dB | 27,80 (7,1) cdA |
| FiltekBF | 23,12 (4,5) cA | 21,9 (7,5) dA |
| Sonic | 40,40 (10,6) bB | 102,31 (20,0) bA |
| SDR + FiltekZ | 31,42 (3,9) bcA | 34,24 (6,9) cA |
The supernatant was submitted to absorbance reading through spectrophotometry in order to quantify the dye content of each solution. For absorbance reading, the spectrophotometer (Beckman DU 65, Instruments, Fullerton, CA, USA) was adjusted to 669 nm wavelength, corresponding to the maximum absorbance of methylene blue. The highest value of spectral absorbance was obtained for each solution. By using ABS-Concentration system, the value of R2 (1) and equation of the line were obtained (y = a + bx). The following regression was obtained: absorbance (y) = 22,759 x(dye concentration) + 0,0011. From this regression, dye concentration was calculated. A line chart was drawn in a Cartesian axes system, inserting the values of dye concentration, in μg/mL, in the abscissa axis and optical density in the ordinate
axis. The linear regression of y on x was obtained to determine the line equation, from which dye concentration was calculated.
After observing data’s normality and equality of variances, microleakage results were submitted to two-way ANOVA and post-hoc Tukey’s test, with significance level at 5%.
RESULTS
Results are presented in Table 2, which demonstrates that, when not submitted to mechanical and thermal aging, FiltekZ showed the highest values of marginal microleakage, followed by Sonic, FiltekBF and finally TetricBF. SDR + FiltekZ results did not differ statistically from Sonic and FiltekBF results.
For groups submitted to mechanical and thermal aging, the highest values of marginal microleakage were also obtained by FiltekZ, followed by Sonic, SDR + FiltekZ and FiltekBF. TetricBF results did not differ statistically neither from SDR + FiltekZ nor from FiltekBF results.
Solely TetricBF and Sonic presented higher marginal microleakage values in aged groups in relation to the not-aged groups.
DISCUSSION
Maintaining marginal integrity over time is essential for a successful restoration. Considering the recent introduction of bulk-fill composites into dental market, this study aimed to evaluate quantitatively the marginal microleakage of restorations of bulk-fill and conventional composites whether or not submitted to mechanical and thermal aging. In order to eliminate bias that could influence on the stress development during polymerization shrinkage [14], the same cavity dimensions (C-factor), adhesive system and light-curing unit were adopted for all materials tested. The type of material dictated its mode of application on the restorative procedure, and the dye penetration was measured by the spectrophotometer technique [15].
As the conventional composite (FiltekZ) showed the highest values of microleakage (p < 0.05), regardless of being submitted to mechanical and thermal aging, the null hypothesis was rejected. This result is contrary to the ones found on the studies of Marí et al, Habib et al and Mosharrafian et al, which evaluated microleakage of conventional and bulk-fill composites but did not find statistically significant differences between them [2,16,5]. According to Hepdeniz and colleagues, marginal sealing ability seems to be affected not only by the characteristics of materials, but also by study design [17]. All studies previously cited
measured the microleakage using an optical microscope. Namely, a single operator subjectively attributed the dye penetration at tooth-restoration interface to a score system based on ISO/ TS 11405:2003. However, such technique may underestimate results, since the evaluation is performed in a bidimensional view, limited to one section of the restoration, which might not correspond to the overall microleakage [3]. Accordingly, composites physical properties may not always coincide with their microleakage assessment.
Furthermore, different to the other composites of bulkfill type, FiltekZ was restored through incremental technique. Studies assessing cuspal deflection on pre-molars [18,19] and third molars [20,21] have shown that placement of multiple increments increases the deformation of restored tooth, leading to greater stress. When the stress generated exceeds the bond strength between adhesive and tooth, microgaps
can be formed [22]. On the other hand, the placement of a single horizontal increment reducing the cusp length not only decreases the area susceptible to deformation (cantilever beam theory), but also constrains both cusps simultaneously during light curing, which further limits the overall mean deflection [19,20]. It should also be highlighted that FiltekZ is composed by triethyleneglycol dimethacrylate (TEGDMA) and polyethylene glycol dimethacrylate (PEGDMA). Although in small quantity, these low molecular weight monomers can increase the mobility in the reaction environment and the density of polymerizable carbon double bonds that can lead to more shrinkage [14,24]. In addition, they are more prone to leaching [25], which may also contribute to microgaps development [23].
Sonic and SDR + FiltekZ showed intermediate means of marginal microleakage (p < 0.05). Sonic is applied through sonicactivation, which makes the material flow during placement. Peutzfeldt and Asmussen reported correlation between composite consistence and marginal adaptation [26]. Accordingly, the more flow the material, the better adapted it should be to the cavity walls [5,12]. Nevertheless, a previous study has shown that Sonic failed to fulfill the requirement of ISO 4049, since the manufacturer states that this composite has adequate depth of cure up to 5-mm increments, while the mean depth of cure found was 3.43 mm [27]. Habib and colleagues, in 2018, also reported lower values of degree of conversion for Sonic restorations at their bottom surfaces [16]. The reason for these results might relies on the fact that Sonic is a composite with high filler content, which to a certain extent, may reduce the passage of light and prejudice the curing process [27]. Consequences on composite physical properties due to inadequate resin polymerization are well described in the literature, such as reduction in the bond strength of the restoration to the tooth, increasing marginal wear and breakdown [3]. Considering that the cavity tested in this study was 5mm deep, the bottom of the restoration not well cured may have contributed to the intermediate values of marginal microleakage of this composite, despite its ability to a better marginal adaptation.
SDR, in turn, is a resin system based on “Stress Decreasing Resin technology” [28]. According to manufactures, the organic matrix comprises on modified urethane dimethacrylate (UDMA) incorporated by a high molecular weight polymerization modulator which is able to control the polymerization kinects [29]. Through a synergic interaction of this stress-relieving monomer with camphorquinone, the gel point is delayed increasing the time for internal stress relaxation, and consequently reducing its polymerization shrinkage [28]. The aliphatic chain of the UDMA monomer is characterized by relative flexibility, which associated to the capability of the imine functional groups (--NH- -) to promote polymerization continuance, improves its degree of conversion [30,24]. All these benefits of SDR may contribute to reduce its polymerization stress. However, considering that microleakage development is a multifactorial phenomenon [16], the composition modifications proposed by the manufacturer for this material might not be enough to contain its volumetric shrinkage due to its increased monomer content. This is in agreement to Benetti et al, who observed higher polymerization shrinkage values for low viscosity bulk-fill resin composites, such as SDR [27], and Alsagob et al, who found higher value of marginal microleakage for this specific material in comparison to another bulk-fill flowable composite and a nanohybrid one [3].
The low values of marginal microleakage obtained by TetricBF (p < 0.05), regardless of being aged, should be highlighted. Although TetricBF is indicated for restorations in increments of up to 4mm, the results obtained by the composite, even used in 5mm increments in this study, can be explained by its composition. According to manufacturer’s information, TetricBF incorporates several types of filler, including the Isofiller, composed of cured dimethacrylates, glass filler and ytterbium fluoride. This specific filler has a low elastic modulus (10 GPa), which favors its action as a “shrinkage stress reliever”, expanding slightly during polymerization and reducing the stress placed on the cavity walls by the standard fillers of high elastic modulus (71 GPa). Namely, volumetric shrinkage and shrinkage stress are reduced. Also, one of TetricBF light initiators, named Ivocerin, a dibenzoyl germanium derivative, allows the composite to be cured at greater depths. Ivocerin is more light-reactive than traditional camphorquinone, increasing polymerization efficiency. In agreement to the characteristics of this material, studies have demonstrated lower values of shrinkage stresses [27,31] and gap formation for 4–6mm depth restorations [22,08].
When submitted to mechanical and thermal aging, FiltekBF also showed the lowest mean marginal microleakage (p < 0.05). FiltekBF composes an organic matrix and inorganic content, which act in combination to decrease polymerization shrinkage. According to manufacturer, the high molecular weight monomer aromatic urethane dimethacrylate (AUDMA) decreases the number of reactive groups in the composite,
which aids to moderate volumetric shrinkage. Also, AFM methacrylate (addition-fragmentation monomers) contains a third reactive site which splits through a fragmentation process during polymerization. This process provides a mechanism for relaxation of polymer network development and subsequent stress relief. Ultimately, FiltekBF presents high filler content, which can, to a certain extent, reduce polymerization shrinkage by increasing the filler:monomer ratio [14,32], and consequently, decrease marginal microleakage. Accordingly, Patel et al compared marginal sealing of three different bulk?fill composite on Class II restorations under in vitro conditions and found that FiltekBF showed the least microleakage and better marginal adaptation [33].
Mechanical and thermal cycling were applied to all composites herein tested. It is important to bear in mind that such methodology simulates the restoration in oral cavity over time. A total of 500 thermal cycles in water with temperatures ranging from 5° C to 55° C are considered an adequate test for dental materials aging, according to ISO standards (TR 11405) [12]. This study applied further 50 thermal cycles and additional mechanical ones in order to properly test the materials’ behavior over time. Considering restorations replacement in clinical practice is partially related to the composite’s features [34], analyzing its properties in face of aging is of prime importance as a possible predictor of quality and possible longevity of the material itself. Regarding the influence of mechanical and thermal aging on marginal microleakage, except for TetricBF and Sonic, no composite presented higher microleakage values when aged (p > 0.05). It should be noticed that periodontal ligament represents an essential structure for stress distribution entailed by load application over teeth [35] and its simulation may have played a role on these results. From compression and strain, this fibrous joint undergoes mechanical adaptation, as load is transferred to
the alveolar bone and stress can be distributed to root surfaces [11,36]. The absorption of occlusal loads may decrease impacts suffered by the contact of maxillary and mandibular teeth [36], such as gaps development and consequently microleakage.
Interestingly, it is worth to note that, although bulkfill composites have presented lower microleakage than conventional composites, regardless of being aged or not, from three bulk-fill composites evaluated, two presented higher microleakage when submitted to mechanical and thermal aging. Herein, the limitations of this study should be pointed out. The number of thermal cycles applied in the aging methodology correspond to less than one year of in vivo test [12]. In addition, only one conventional composite was analyzed; and finally, more contemporary tests, such as nanoinfiltration, could be applied as an alternative to test marginal infiltration. Thus, further studies of long-term aging of bulk-fill restorations, including more composites and sophisticated methods, are needed to clarify whether and how far their performance is maintained.
CONCLUSIONS
Bulk-fill composites restorations presented lower marginal microleakage than conventional composite restorations, regardless of being aged or not. However, bulk-fill composites were more prone to the effects of aging than conventional composite.
ACKNOWLEDGEMENTS
This work was supported by the State of São Paulo Research Foundation (FAPESP) (No. 2015/24373-6). The authors are grateful to Mr. Felipe Joia for his technical assistance with spectrophotometer. The authors do not have any financial interest in the companies whose materials are included in this article.
A: Immersion of bovine tooth root in melted wax. B: Fixation of the tooth through radiographic film with sticky wax; positioning of the set on perforated wood board; polystyrene resin insertion into PVC pipe. C: Removal of tooth from polystyrene resin matrix and removal of root wax film. D: Polyether insertion and reinsertion of the tooth in the matrix. E: Transverse sectioning of tooth crown; obtaining wide incisal surface. F: Cavity preparation and restoration. G: Protection of the sample with nail varnish, except for the tooth restoration interface; immersion of the sample in 2% methylene blue dye; Sectioning and grinding of tooth-restoration interface blocks; immersion of the obtained powder in absolute alcohol. * Simulation of periodontal ligament.
Means followed by distinct letters (uppercase in horizontal and lowercase in vertical) differ from each other (p≤0.05).
REFERENCES
1. Chandrasekhar V, Rudrapati L, Badami V, et al. Incremental techniques in direct composite restoration. J Conserv Dent. 2018; 20: 386-391.
2. Marí LG, Gil AC, Puy CL. In vitro evaluation of microleakage in Class II composite restorations: High-viscosity bulk-fill vs conventional composites. Dent Mater J. 2019 Sep 27; 38: 721–727.
3. Alsagob EI, Bardwell DN, Ali AO, et al. Comparison of microleakage between bulk-fill flowable and nanofilled resin-based composites. Interv Med Appl Sci. 2018; 10: 102–109.
4. Borges AL, Borges AB, Xavier TA, et al. Impact of quantity of resin, C-factor, and geometry on resin composite polymerization shrinkage stress in Class V restorations. Oper Dent. 2014; 39: 144-151.
5. Mosharrafian S, Heidari A, Rahbar P. Microleakage of Two Bulk Fill and One Conventional Composite in Class II Restorations of Primary Posterior Teeth. J Dent (Tehran). 2017; 14: 123–131.
6. Son SA, Park JK, Seo DG, et al. How light attenuation and filler content affect the microhardness and polymerization shrinkage and translucency of bulk-fill composites? Clin Oral Investig. 2016; 21: 559-
565.
7. Van Ende A, De Munck J, Lise DP, et al. Bulk-Fill Composites: A Review of the Current Literature. J Adhes Dent. 2017; 19: 95-109.
8. Fronza BM, Rueggeberg FA, Braga RR, et al. Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent Mater. 2015; 31: 1542-1551.
9. Pfeifer CS. Polymer-Based Direct Filling Materials. Dent Clin North Am. 2017; 61: 733–750.
10. Cidreira Boaro LC, Pereira Lopes D, de Souza ASC, et al. Clinical performance and chemical-physical properties of bulk fill composites resin —a systematic review and meta-analysis. Dent Mater. 2019; 35:
e249–264.
11. Soares CJ, Pizi EC, Fonseca RB, et al. Influence of root embedment material and periodontal ligament simulation on fracture resistance tests. Braz Oral Res. 2005; 19: 11-16.
12. Pereira R, Lima DANL, Giorgi MCC, et al. Evaluation of Bond Strength, Nanoleakage, and Marginal Adaptation of Bulk-fill Composites Submitted to Thermomechanical Aging. J Adhes Dent. 2019; 21: 255- 264.
13. Hernandes NM, Catelan A, Soares GP, Ambrosano GM, Lima DA, Marchi GM, Martins LR, Aguiar FH. Influence of flowable composite and restorative technique on microleakage of class II restorations. J Investig Clin Dent. 2014; 5: 283-8.
14. Braga RR, Ballester RY, Ferracane JL. Factors involved in the development of polymerization shrinkage stress in resin-composites: a systematic review. Dent Mater. 2005; 21: 962-970.
15. Aguiar FH, Santos AJ, Groppo FC, et al. Quantitative evaluation of marginal leakage of two resin composite restorations using two filling techniques. Oper Dent. 2002; 27: 475-479.
16. Habib ANA, Waly GH. The degree of conversion and class II cavity microleakage of different bulk-fill composites placed with different restorative techniques. FDJ. 2018; 4: 231-238.
17. Hepdeniz OK, Ermis RB. Comparative evaluation of marginal adaptation and microleakage of low-shrinking composites after thermocycling and mechanical loading. Niger J Clin Pract. 2019; 22:
633–641.
18. Versluis A, Douglas WH, Cross M, et al. Does an incremental filling technique reduce polymerization shrinkage stresses? J Dent Res. 1996; 75: 871-878.
19. Moorthy A, Hogg CH, Dowling AH, et al. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resinbased composite base materials. J Dent. 2012; 40: 500-505.
20. McHugh LEJ, Politi I, Al-Fodeh RS, et al. Implications of resin-based composite (RBC) restoration on cuspal deflection and microleakage score in molar teeth: Placement protocol and restorative material.
Dent Mater. 2017; 33: e329-e335.
21. Politi I, McHugh LEJ, Al-Fodeh RS, et al. Modification of the restoration protocol for resin-based composite (RBC) restoratives (conventional and bulk-fill) on cuspal movement and microleakage score in molar
teeth. Dent Mater. 2018; 34: 1271-1277.
22. Sampaio CS, Fernández Arias J, Atria PJ, et al. Volumetric polymerization shrinkage and its comparison to internal adaptation in bulk fill and conventional composites: A μCT and OCT in vitro analysis.
Dent Mater. 2019; 1–8.
23. Nalçaci A, Uluosoy N, Atakol O. Time-based elution of TEGDMA and BisGMA from composite cured with LED, QTH and high-intensity QTH light. Oper Dent. 2006; 31: 197-203.
24. Pereira R, Giorgi MCC, Lins RBE, et al. Physical and photoelastic properties of bulk-fill and conventional composites. Clin Cosmet Investig Dent. 2018; 10: 287-296.
25. Gajewski VE, Pfeifer CS, Fróes-Salgado NR, et al. Monomers used in resin composites: degree of conversion, mechanical properties and water sorption/solubility. Braz Dent J. 2012; 23: 508-514.
26. Peutzfeldt A, Asmussen E. Determinants of in vitro gap formation of resin composites. J Dent. 2004; 32: 109-115.
27. Benetti AR, Havndrup-Pedersen C, Honoré D, et al. Bulk-fill resin composites: polymerization contraction, depth of cure and gap formation. Oper Dent. 2015; 40: 190-200.
28. Ilie N, Hickel R. Investigations on a methacrylate-based flowable composite based on the SDR technology. Dent Mater. 2011; 27: 348-355.
29. Jang JH, Park SH, Hwang IN. Polymerization shrinkage and depth of cure of bulk-fill resin composites and highly filled flowable resin. Oper Dent. 2015; 40: 172-180.
30. Fonseca AS, Labruna Moreira AD, de Alburquerque PP, et al. Effect of monomer type on the CC degree of conversion, water sorption and solubility, and color stability of model dental composites. Dent Mater.
2017; 33: 394-401.
31. El-Damanhoury H, Platt J. Polymerization shrinkage stress kinetics and related properties of bulk-fill resin composites. Oper Dent. 2014; 39: 374-382.
32. Kleverlaan CJ, Feilzer AJ. Polymerization shrinkage and contraction stress of dental resin composites. Dent Mater. 2005; 21: 1150-1157. 33.
33. Patel MC, Bhatt RK, Makwani DA, et al. Comparative evaluation of marginal seal integrity of three bulk-fill composite materials in class II cavities: an in vitro study. Adv Hum Biol. 2018; 8: 201-205.
34. Demarco FF, Corrêa MB, Cenci MS, Moraes RR, Opdam NJ. Longevity of posterior composite restorations: not only a matter of materials. Dent Mater. 2012; 28: 87-101.
35. Rosentritt M, Fürer C, Behr M, et al. Comparison of in vitro fracture strength of metallic and tooth-coloured posts and cores. J Oral Rehabil. 2000; 27: 595-601.
36. Lin JD, Jang AT, Kurylo MP, et al. Periodontal ligament entheses and their adaptive role in the context of dentoalveolar joint function. Dent Mater. 2017; 33: 650-666.







































































































































{kind=link}