Through Steel and Bone: Navigating a Difficult Airway after an Unusual Robotic‑Arm Penetration of the Mandible
- 1. Department of Anesthesiology, Hospital of Lucerne, Switzerland
- 2. University of Lucerne, Switzerland
Abstract
Penetrating injuries to the face and neck are a relatively rare condition that requires immediate airway assessment. In the presence of predictors of a difficult airway, Awake Fiberoptic Intubation (AFI) provides controlled access while preserving spontaneous breathing and protective reflexes. We present the case of a 54-year-old patient with a penetrating mandibular injury caused by an industrial robotic arm. Preclinically, airway management was not performed due to adequate spontaneous breathing. In the trauma room, due to the injury pattern accompanied by severe craniomandibular dysfunction, the decision was made to perform awake fiberoptic intubation in a sitting position. This case demonstrates the feasibility of AFI under challenging conditions, particularly in cases of unknown injury patterns, lack of patient cooperation, and unconventional positioning.
Keywords
• Awake Fiberoptic Intubation; Difficult Airway Management; Penetrating Facial Trauma; Industrial Accident; Multidisciplinary Trauma Management
Citation
Jungck L, Konrad C, Arnold T, Schöb M, Herr R (2026) Through Steel and Bone: Navigating a Difficult Airway after an Unusual Robotic?Arm Penetration of the Mandible. Ann Otolaryngol Rhinol 13(3): 1390.
ABBREVIATIONS
AFI: Awake fiberoptic Intubation; HFNO: High-Flow Nasal Oxygen; MAD: Mucosal Atomization Device
INTRODUCTION
Penetrating injuries to the face and neck are a rare but potentially life-threatening condition [1]. Airway management in patients with maxillofacial trauma is particularly challenging, as multiple factors such as edema, bleeding, limited mouth opening, loss of bony support structures, and the risk of regurgitation and aspiration can complicate airway management [2]. The decision between rapid sequence intubation – the rapid induction of anesthesia with a hypnotic and a fast-acting muscle relaxant to minimize the risk of aspiration in non- fasting patients – and awake fiberoptic intubation is a clinical judgement that depends on the patient’s condition, available resources, and the team’s expertise [2]. Awake fiberoptic intubation is considered the gold standard for anticipated difficult airways. However, techniques for securing the airway in conscious patients remain underutilized [3].
We report on a 54-year-old patient who sustained a severe penetrating injury to the right side of his face and neck caused by an industrial robot arm. This case illustrates the challenges of securing the airway in an extremely uncooperative patient with an unclear injury pattern, as well as the decision-making process required to successfully secure the airway.
CASE PRESENTATION
A 54-year-old patient with no relevant pre-existing conditions suffered a severe workplace accident involving a robotic arm. The robotic arm, equipped with a pair of pliers at its tip, pierced the patient’s head and neck from the side. The patient was initially trapped and was freed by coworkers. The main arm of the robot was removed by workshop staff. A metal part weighing approximately 2 kg, equipped with a pair of pliers, remained embedded approximately 8cm deep in the lower jaw structures and protruded about 20 cm from the body. The patient held the foreign body in place on his own and refused any assistance. Upon the arrival of the emergency medical services, the patient presented with a potentially compromised airway. The mouth and nose were bloody, and the mouth could only be opened about 1 cm. Under nasal oxygen administration, the patient was clammy and tachycardic. Neurologically, the patient appeared to be in a state of severe psychological distress, uncooperative, and verbally aggressive. Based on a risk-benefit assessment, pre- hospital airway management was not performed. Intravenous analgesia and anxiolysis were administered in divided doses, with a cumulative dose of 0.3 mg fentanyl, 20 mg esketamine, and 2 mg midazolam. The patient was transported to the trauma resuscitation room at the nearest trauma center (Figure 1).

Figure 1 Photograph demonstrating the penetrating robotic arm to the right mandibular angle and lateral neck region. The patient is seated leaning forward, manually stabilizing the foreign body.
Upon arrival in the emergency room, the patient was seated on the ambulance stretcher, with the metal forceps of a robotic arm positioned at the right angle of his neck and jaw, holding the foreign object in place with both hands. The structured initial assessment was conducted according to the XABCDE protocol. No critical external bleeding was observed. The airways appeared clear as far as could be assessed, with spontaneous breathing intact; however, instability of the cervical spine could not be ruled out due to the mechanism of the accident. Auscultation of the lungs revealed symmetrical ventilation with a peripheral oxygen saturation of 98% under oxygen insufflation. Hemodynamically, the patient presented with hypertension and a normal heart rate. Neurologically, the patient was awake and responsive with a Glasgow Coma Scale score of 15, but markedly uncooperative. The pupils were prompt and isocoric with normal light reflexes; the extremities were, as far as could be assessed, freely movable; there were no signs of a focal neurological deficit. A full-body examination revealed no evidence of further trauma-related injuries. All relevant specialties were present in the trauma room: Emergency Medicine, anesthesiology, otolaryngology, oral and maxillofacial surgery, neurosurgery, and vascular surgery.
Given the anatomical distortion caused by the penetrating trauma, the severely limited mouth opening, the inability to predict the airway anatomy, and the risk of airway obstruction during induction of anesthesia, the decision was made to secure the primary airway via awake nasal fiberoptic intubation with the patient in a sitting position.
The following equipment was prepared for awake fiberoptic intubation: a flexible bronchoscope with an outer diameter of 5 mm, a reinforced endotracheal tube with an inner diameter of 6.5 mm, as well as tubes in smaller sizes as backup, topical anesthesia, and a suction system. Monitoring was performed using pulse oximetry and ECG; the blood pressure cuff was still not tolerated. Intubation was performed with tracheotomy equipment on standby.
Therapeutic Intervention: Awake fiberoptic intubation
The patient was seated on the ambulance stretcher and, due to pain and anxiety, could not tolerate any change in position. He was clutching the foreign object tightly and appeared very anxious. Topical preparation of the nasal airway was performed according to local Standard Operating Procedures [4] using a mixture of 4% lidocaine and 10% cocaine via Mucosal Atomization Device (MAD); topical anesthesia of the oral airway was performed with 4% lidocaine. Sedation was administered with an infusion of remifentanil. Due to the severely limited mouth opening of less than 1 cm, the decision was made to perform nasal intubation. The patient remained in a seated position. Vomiting occurred during fiberoptic endoscopy of the nasal airway. Following this incident, the fiberoptic scope was successfully repositioned without issue. Successful probing into the trachea was performed under direct visualization, followed by advancement of the tube into the endotracheal space. Fiberoptic endoscopy revealed a clear nasal passage on the left, no evidence of endonasal injuries; the epipharynx was clear; the posterior pharyngeal wall showed a trace of blood but no open injuries. The larynx presented with an intact mucosa, no redness or swelling; there was no swelling of the epiglottis, the vocal cords and trachea appeared normal. Correct tube placement was confirmed by capnography, followed by intravenous induction of anesthesia. Airway management was performed by two experienced anesthesiologists.
The subsequent Computed Tomography (CT) scan of the skull and neck revealed a right- sided buccal foreign body perforation with the tips of the foreign body at the sphenoid bone and lateral to the mandibular ramus. A fracture of the right mandibular neck with medial displacement was found, as well as a slightly displaced fracture of the lateral lamina of the right pterygoid process. In addition, a fracture of the right nasal bone was diagnosed. There were no clear indications of injuries to the vascular structures. There was no intracranial hemorrhage or skull fracture, and the cervical spine appeared intact. There were no signs of tracheal injury (Figure 2).
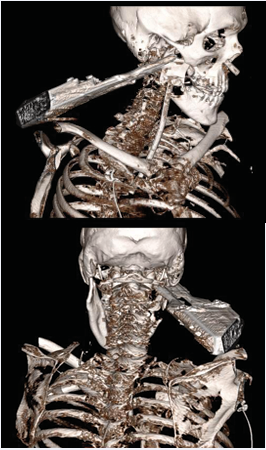
Figure 2 CT scan after AFI showing the penetrating robotic arm.
The patient was transferred to the operating room for controlled extraction of the foreign body. Postoperatively, the patient was transferred to the intensive care unit. Extubation was performed without complications, and the patient was transferred to the general ward on the first postoperative day. The subsequent course was uneventful. On the fifth postoperative day, the patient was discharged; right facial nerve palsy and right V2/V3 hypoesthesia persisted. Osteosynthesis of the mandible was performed subsequently.
DISCUSSION
This case describes the successful use of AFI in a patient with a severe penetrating neck/face injury caused by a robotic arm. The case illustrates the importance of structured decision-making in securing the airway in the context of complex trauma with predictors of a difficult airway.
The decision to use AFI in this case was based on several established indications: The patient presented with a mouth opening of less than 1 cm, which made both direct laryngoscopy and video laryngoscopy impossible. Additionally, due to the penetrating foreign body’s proximity to the major neck vessels, there was a risk of airway obstruction caused by bleeding or hematoma. In our case, maintaining spontaneous breathing was essential, as the extent of the airway injury was unknown. Fiberoptic endoscopy allowed for direct visualization of the injury.
AFI has a very high success rate of 99.6% combined with a low complication rate [5]. It should be noted that the procedure takes longer; the median duration of AFI is approximately 8 minutes longer than intubation following induction of anesthesia [6]. In a situation such as that of our patient, this time requirement was accepted and justified by increased safety. A failure rate of 3.5%, most commonly due to tube displacement after induction of anesthesia, patient agitation, inability to advance the tube, and airway bleeding, has been described [7].
Visualization can be significantly impaired, particularly in cases of facial trauma with pre- existing bleeding in the airway. In addition, bronchoscopy can induce bleeding; in particular, bleeding has been observed in up to 10% of cases during nasal fiberoptic intubation [8]. Mastering FOI requires structured training and a sufficient number of procedures to achieve competence. The literature indicates that an average of 15 procedures is required to achieve competence and confidence, while at the same time a concerning lack of exposure is documented [9]. Our case highlights the need for sufficient exposure and structured training in fiberoptic intubation.
The use of High-Flow Nasal Oxygen (HFNO) during AFI has become increasingly important in recent years. HFNO delivers warmed, humidified oxygen at flow rates of up to 60 L/min and offers several physiological benefits: flushing of the anatomical dead space, reliable delivery of high FiO? concentrations, generation of low Positive End Exspiratory Pressure (PEEP), and reduction of respiratory effort [10]. The soft nasal cannulas allow for continuous oxygenation while the fiberscope is being passed.
A key aspect of airway management in penetrating facial and neck trauma is anticipating the potential failure of the primary intubation strategy [11]. In the present case, AFI was chosen, with the advantage that, with the patient remaining conscious and breathing spontaneously, the patient’s own airway patency is maintained, and time can be gained for alternative strategies. Switching to oral fiberoptic intubation or video laryngoscopy was not an option in our case due to an extremely small mouth opening of <1 cm, nor was the use of a supraglottic airway device. In the event of a “Cannot Intubate, Cannot Oxygenate” situation, front-of-neck access would have been the only option for securing the airway.
This was anticipated, and the patient was intubated with tracheotomy equipment and the ENT team on standby.
Unique aspects of the case:
- Injury caused by a robotic arm is a rare occurrence; the injury pattern was unpredictable; the 2 kg robotic arm was still in place.
- Sitting position: The patient was unable to tolerate a change in position due to pain and the presence of the foreign object. While head extension is recommended for elective AFI [12], case reports show that AFI can also be successfully performed in unconventional positions [13]. This demonstrates the flexibility and adaptability of AFI in challenging clinical situations.
- Uncooperative patient: The patient’s psychological distress and uncooperativeness posed an additional challenge. Although a lack of patient cooperation constitutes a relative contraindication for AFI [11], successful intubation was achieved through adequate topical anesthesia and sedation.
CONCLUSION
This case demonstrates the successful use of awake fiberoptic intubation in a patient with a severe penetrating facial and neck injury caused by a robotic arm. AFI allowed for safe airway management while preserving spontaneous breathing and protective reflexes. Early airway management using AFI enabled safe diagnostic evaluation and surgical treatment.
REFERENCES
- Burgess CA, Dale OT, Almeyda R, Corbridge RJ. An evidence based review of the assessment and management of penetrating neck trauma. Clin Otolaryngol. 2012; 37: 44-52.
- Jain U, McCunn M, Smith CE, Pittet JF. Management of the traumatized airway. Anesthesiology. 2016; 124: 199-206.
- Heidegger T. Management of the difficult airway. N Engl J Med. 2021; 384: 1836-1847.
- Standard Operating Procedures.
- Pirlich N, Berk A, Hummel R, Schmidtmann I, Epp K, Kriege M, et al. Awake tracheal intubation in routine airway management: A retrospective analysis in a tertiary centre. PLoS One. 2024; 19: e0299071.
- Joseph TT, Gal JS, DeMaria S Jr, Lin HM, Levine AI, Hyman JB. A Retrospective Study of Success, Failure, and Time Needed to Perform Awake Intubation. Anesthesiology. 2016; 125: 105-114.
- Karlsen KAH, Gisvold SE, Nordseth T, Fasting S. Incidence, causes, and management of failed awake fibreoptic intubation-A retrospective study of 833 procedures. Acta Anaesthesiol Scand. 2023; 67: 1341-1347.
- Woodall NM, Harwood RJ, Barker GL. Complications of awake fibreoptic intubation without sedation in 200 healthy anaesthetists attending a training course. Br J Anaesth. 2008; 100: 850-855.
- Cai X, Yue M, Liu X, Zhang L, Wu S, Shen W, et al. Learning curve for flexible bronchoscope-guided orotracheal intubation for anesthesiology residents: A cumulative sum analysis. PLoS One. 2023; 18: e0288617.
- Spoletini G, Alotaibi M, Blasi F, Hill NS. Heated humidified high-flow nasal oxygen in adults: Mechanisms of action and clinical implications. Chest. 2015; 148: 253-261.
- Ahmad I, El-Boghdadly K, Bhagrath R, Hodzovic I, McNarry AF, Mir F, et al. Difficult Airway Society guidelines for Awake Tracheal Intubation (ATI) in adults. Anaesthesia. 2020; 75: 509-528.
- Liu Z, Zhao L, Ma Z, Liu M, Qi X, Jia Q, et al. Effects of head positions on awake fiberoptic bronchoscope oral intubation: A randomized controlled trial. BMC Anesthesiol. 2021; 21: 176.
- Yang J, Zou F, Ma G. Awake fiberoptic intubation of a patient with severe multiple trauma in prone position: A case report. BMC Anesthesiol. 2024; 24: 245.








































































































































