The Mailbox-Slot Pericranial Flap for Coverage of an Internal Carotid Artery in the Sphenoid Sinus
- 0. These authors contributed equally to this project and should be considered co-first authors
- 1. Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital of Ulm, Germany
- 2. Department of Diagnostic and Interventional Radiology Section Neuroradiology, University Hospital of Ulm, Germany
ABSTRACT
Objectives: A potential risk of paranasal sinus tumor surgery and postoperative radiation is an exposed internal carotid artery (ICA), which can lead to life threatening, arterial bleeding. Various treatment approaches are possible.
Methods: We present the case of a patient with widely exposed internal carotid artery due to ongolocigal resection and following radiotherapy, who has been treated successfully with a “Mailbox-slot” pericranial flap in our department.
Results: Within a follow-up of nine months after surgery the patient did not suffer any further bleedings. The flap showed regular healing conditions with fibrous tissue coverage of the ICA.
Conclusion: This case report details that the “Mailbox-slot” approach is one viable technique to cover defects of the ICA especially in complicated cases with anticipated limited wound healing.
KEYWORDS
• Internal carotid artery haemorrhage
• Pericranial flap
• Mailbox-slot approach
• Skull base defect reconstruction
• Galea Flap
CITATION
Scheithauer MO, Lindemann J, Schmitz B, Hoffmann TK, Trainotti S, et al. (2022) The Mailbox-Slot Pericranial Flap for Coverage of an Internal Carotid Artery in the Sphenoid Sinus. Ann Otolaryngol Rhinol 9(2): 1285.
ABBREVIATIONS
ICA: Internal Carotid Artery, PCF: Pericranial Flap
INTRODUCTION
Several techniques to cover defects of the internal carotid artery (ICA) are described in the current literature [1]. However, particularly complicated situations may arise after previous radiation therapy.
CASE PRESENTATION
We report about a 59 year-old male patient who received a radical resection of an adenoid-cystic carcinoma of the right ethmoid and sphenoid sinus eight years ago. Due to recurrent disease a C12 heavy ion radiation was performed three times within six years. Two years after radiation therapy the patient was admitted as an emergency to the hospital with epistaxis. Initially, the bleeding was severe but nearly stopped, when the patient presented himself in the hospital. CT-angiography revealed an exposed internal carotid artery (ICA) within the remnants of the right sphenoid sinus (Figure 1).
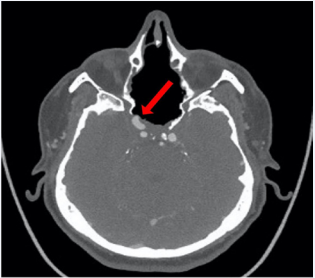
Figure 1: CT Angiography of the intracranial vessels. The ICA on the right side within the former sphenoid sinus has no bony or soft tissue coverage (red arrow).
A bony covering of the ICA was absent. During endoscopy an “empty nose” with a missing posterior nasal septum could be observed. The mucosa was dry and crusty. There was an intensive foetor suggesting a severe infection due to exposed bone. A clear pulsation at the lateral aspect of the right sphenoid sinus could be seen. Tumor recurrence was not obvious. In order to prevent the rupture of the arterial wall due to secondary infection, surgical therapy was chosen. In a regular anatomical endonasal site with an intact septum the method of choice would have been the use of a pedicled septal flap covering the ICA. Alternatively, a free muscle patch could be used, but with minor success, because of the impaired healing due to radiation therapy in the past [2]. Three flow-diverters were introduced in the right ICA by an interventional neuroradiologist preventing an early recurrent blow-out. Additionally, a direct carotid-cavernous-sinus fistula originating at the carotid lesion was coiled from the venous side using a transfemoral, transvenous approach through the inferior petrosal sinus. Due to preoperative radiation therapy the only well perfused tissue available in the head region was a pericranial flap (PCF), due of its distance to the radiation field. The flap was transferred to the sphenoid sinus via a gate directly through the ipsilateral frontal sinus, which makes the existence of a ventilated frontal sinus cavity and a mandatory condition for this approach. In the present case the CT-scan of the paranasal sinus system revealed an extended frontal sinus. First published in 2016, the so called “Mailbox-slot” approach is an ideal access to create a safe route to the skull base corridor [3]. The operation starts with a bicoronal incision. Superficially of the PCF the scalp is mobilized anteriorly and posteriorly in a blunt dissection. Anteriorly the preparation ends at the nasal root and the supraorbital rims preserving the supraorbital nerve (Figure 2A).
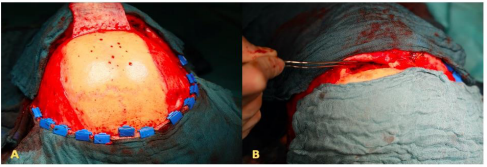
Figure 2: A) Bicoronal incision with pericranial flap. B) Pull through maneuver through the frontal sinus.
An osteoplastic approach to the frontal sinus cavity is performed. A diamond burr is used to create the actual connection from the sinus to the ventral skull base. The interfrontal septum, the complete floor of the frontal sinus and the dorsal parts of the nasal septum are removed. Now the length of the pericranial flap is measured under consideration of the cranial dissection line of the osteoplastic sinus approach as pivot line. Usually a length of about 14 to 16 cm is sufficient to cover the exposed ICA. A flap-width of four to five centimeter is necessary. Once the flap is harvested, it is turned and transferred into the frontal sinus and endoscopically positioned over the exposed ICA (Figure 2B and 3A).
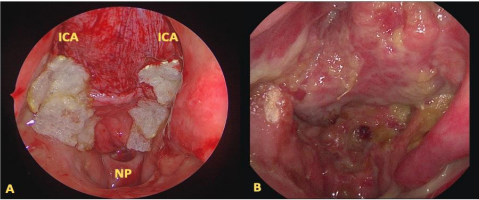
Figure 3: A) Endoscopically positioned pericranial flap fixated with fibrin glue and TachoSil. B) Postoperative situation after 6 months. ICA: Internal Carotid Artery, NP: Nasopharynx
The flap is kept in place by TachoSil, fibrin glue and nasal packings, which are endoscopically positioned. The bony part of the frontal sinus wall is drilled out at its cranial border to reassure a passage of the flap without compressing the pedicle, giving the approach its peculiar name. Afterwards the fragment is readapted and fixed with titanium miniplates and the scalp is realigned. The patient described in this report did not have further bleedings within a follow-up of nine months after surgery. The flap showed regular healing conditions with fibrous tissue coverage of the ICA (Figure 3B) and no severe signs of infection.
DISCUSSION
A widely exposed ICA within the sphenoid sinus due to radical surgical resections and radiotherapy must not be left untreated. In our patient the situation was even more delicate as no sufficient wound healing could be expected due to previous radiotherapy. Whenever possible a pedicled flap from the anatomical neighborhood, for example a naso-septal flap, would be the first choice [4]. However, a missing nasal septum or a huge septal perforation will prevent harvesting a naso-septal flap. Moreover, previous resections of the nasal septum or a prior wide sphenoidotomy preclude its use. In our presented patient, even the turbinates were completely missing, so an inferior turbinate flap could not be used. The use of free grafts (e.g. muscle, fat, and fascia) is no option due to the radiated area and the anticipated limited wound healing. Generally speaking free flaps, as discussed in a publication from Hoffmann et al. are a safe alternative, but technically very complex [2]. Therefore, the only surgical option in this situation was the PCF as depicted above. According to anatomic-radiological studies of Santamaria et al., the maximum length of the pericranial flap is about 19,4 cm covering a surface of 121,5 cm2 [5]. The authors summarized, that the PCF provides enough surface area to reconstruct all possible defects of the ventral and median skull base. The “Mailbox-slot” approach compared to the resection of the nasal bones or the subfrontal extradural approach is a technically easy and quick access. Possible collateral damage is negligible.
CONCLUSION
The “Mailbox-slot” approach is a direct route for the PCF into the skull base corridor. Length and width of the flap are suitable to cover extended dural defects, seal cerebrospinal fluid leaks or covering an exposed ICA preventing life-threatening hemorrhage. Disadvantages are the nasal dressing for several days and the postoperative anosmia. However, the flap can be harvested within a short time and its secure perfusion provides reliable healing even in complicated cases.







































































































































