Chronic Allergic Fungal Sinusitis with Atopic Dermatitis with Erythroderma over Entire Skin Surface Successfully Treated with FESS, Cyclone Amphotericin Irrigation, Medical, and Environmental Management
- 1. Sinusitis Wellness, Atlanta, USA
- 2. East Carolina University-Brody School of Public Health, USA
ABSTRACT
Exposure to molds in the indoor environment and in the paranasal sinuses and other parts of the body can cause a wide range of health problems, including sinusitis, asthma, dermatitis, and chronic fatigue. Here we present a 23-year-old female patient who experienced many years of severe allergic fungal sinusitis (AFS) with polyps and atopic dermatitis, along with severe fatigue, memory loss, weakness, muscle and joint pain, insomnia, and shortness of breath after living in a mold-infested recreational vehicle and having fungi in the sinuses. Pre-operative treatment with antifungal medication nasal irrigation with saline, nutritional supplements, and avoidance of mold did not improve her AFS or atopic dermatitis. Following treatment with endoscopic sinus surgery and Cyclone Amphotericin-Birrigation, the patient’s dermatitis resolved dramatically in only 6 days, along with the AFS and many of her other symptoms.
This case study suggests that exposure to mycotoxins, produced by both the indoor environment and by fungi growing in the sinuses, can produce a wide range of health effects, including sinusitis, dermatitis, chronic fatigue, cognitive impairment, neuropsychiatric signs, and many other symptoms. A multi-faceted treatment regime of endoscopic nasal surgery, indoor environmental testing/control, and medical/hormonal/nutritional treatment can thus potentially improve many health conditions. TAP testing a patient’s clothing for mold with an SDA agar mold screening plate and urine mycotoxin testing can help direct attention to the environmental source of exposure and improve long-term outcome.
KEYWORDS
• Atopic dermatitis
• Mycotoxins
• Functional endoscopic sinus surgery (FESS)
• Amphotericin-B Cyclone irrigation
• Chronic sinusitis
• Microbial volatile organic compounds(MVOCs)
• Fungal sinusitis
• Mycotoxicosis
• Mold poisoning Abstract
• Mold toxicity
CITATION
Dennis D, Curtis L (2022) Chronic Allergic Fungal Sinusitis with Atopic Dermatitis with Erythroderma over Entire Skin Surface Successfully Treated with FESS, Cyclone Amphotericin Irrigation, Medical, and Environmental Management. Ann Otolaryngol Rhinol 9(2): 1286.
INTRODUCTION
Fungal exposure is common in rhinosinusitis patients, with one study reporting 94 out of 101 (93%) consecutive chronic rhinosinusitis surgical patients being diagnosed with fungal chronic rhinosinusitis [1]. More than a hundred studies have reported that heavy exposure to indoor molds and their allergens and mycotoxins can cause a wide range of adverse health effects [2-4], especially asthma [3,5] sinusitis [6,7] chronic fatigue [8-12] neurological/neuropsychiatric problems [10,13- 15] and hormonal deficiencies [9]. A meta-analysis of 31 indoor air studies reported that visible mold (EE 1.82, 95 % CI 1.56- 2.12) and mold odor (EE 2.18, 95 CI 1.76-2.71) were associated with a greater risk of the development of rhinitis/sinusitis [6]. Dennis et al., described a group of 79 patients with a history of documented indoor mold exposure who presented with rhinitis, chronic fatigue, and endocrine problems, including 81% with hypothyroidism and 51% with growth hormone deficiency [9].
When environmental mycotoxins enter the nose, the highest concentration is found in the ethmoid sinus mucosa. The environmental air contains a “soup” of three items: mold spores, mycotoxins (of which there are over 400 [16], and microbial volatile organic compounds (MVOCs). Once in the moist environment of the sinuses, the mold spores become an internal manufacturing facility for more mycotoxins and MVOCs such that illness may persist within a patient’s body even in a mold-free environment. MVOCs can penetrate sheetrock and wood and can go through plastic. Thus, much like the intoxication inherent when glue is inhaled and the chemicals enter the brain causing cognitive dysfunction (brain fog), and neuropsychiatric symptoms, MVOCs can also cross the blood-brain barrier and cause a number of neurological symptoms.
A US study found that mycotoxins, specifically trichothecenes, aflatoxins, and ochratoxins, could be detected in nasal secretions and sputa in patients who had been exposed to molds in their environment [17]. Case series have been presented of patients exposed to water-damaged indoor environments who had measurable levels of mycotoxins in their urine and/or nasal mucosa. These patients all improved following endoscopic sinus surgeries, reductions in indoor mold exposure, and treatment with oral/nasal or nebulized antifungal drugs and neurotherapy [18,19].
Exposure to fungal allergens and toxins can also increase risk of dermatitis and eczema. One 2021 study of 100 atopic dermatitis patients reported that skin sensitization to allergens from fungi commonly found in indoor environments or in/ on humans, including Alternaria, Cladosporium, Penicillium, Aspergillus, and Malassezia, were more common than in patients with no atopic dermatitis [20]. Rhinitis/sinusitis and eczema/ dermatitis frequently co-exist [21], with one study reporting that eczema was present in 21 out of 94 (22%) patients with chronic sinusitis [22].
A number of other studies have also linked exposure to indoor environments with mold and/or moisture damage to significantly higher rates of eczema and related skin problems. A study of 10,851 preschool children in Sweden reported skin eczema rates overall of 18.7%, with presence of visible dampness (OR 1.35, 95% CI 1.15-1.72) being associated with significantly higher rates of childhood skin eczema [23]. A NW China study of 8,153 preschool children reported that maternal residential exposure to mold or moisture was associated with significantly higher risk of eczema development (OR 1.53, 95% CI 1.17-2.00) [24]. A South Korean study of 52 homes of atopic dermatitis patients reported that presence of moisture damage in homes was associated with significantly increased risk of moderate to severe atopic dermatitis (OR 14.52, 95% CI 1.75-121.13, p=0.0025) [25]. A Finnish study reported that skin rashes were seen in 15 out of 47 (32%) students in a water-damaged school as compared to 0 of 56 (0%) control students (p <0.001) [14]. Curtis et al., reported that skin rashes were seen in 13 of 48 (27%) adult subjects exposed to indoor mold [2].
Environmental and medical management of mold-related sinus problems can often produce considerable improvement in patients’ symptoms. Resolution of rhinosinusitis was seen in 93% (41 of 45) of the Dennis patients reported above who were also able to lower their indoor mold concentrations and who received treatment with nasal saline irrigations, antifungal and antibiotic sprays, and appropriate hormone replacement and nutritional supplements [9]. Dennis et al., also reported large and significant improvement in a wide range of symptoms including neuropsychiatric deficits in a case series of 3 patients treated with standard FESS surgery, Cyclone irrigation with voriconazole, nutritional and hormonal treatment, and reduced exposure to molds and other toxins and allergens [26].
CASE PRESENTATION
This case reports on a 23-year-old woman with severe skin rashes over her entire body along with chronic fatigue and a number of other serious health problems. The woman improved dramatically in just 6 days postoperatively following treatment with Functional Endoscopic Sinus Surgery (FESS) of all eight sinuses and Cyclone (Stryker) irrigation of all sinuses with Amphotericin-B. Pre-operative environmental controls, avoidance, and medical therapy to remove the mycotoxins using Oxygen, Glutathione, Opticleanse to detoxify the liver, and Intramax liquid vitamins bound to carbon to help remove toxins were not effective in relieving the allergic fungal sinusitis with polyps or the severe atopic dermatitis. Three partial relapses occurred between November 4, 2021, and December 7, 2021, which were successfully treated without further surgery by injecting maxillary sinus with Amphotericin-B, Kenalog 20, and Xylocaine 1% with epinephrine.
HISTORY
A 23-year-old woman presented with a history of atopic dermatitis (eczema) over the entire body with skin peeling on every surface including the ear canals for at least four years. The symptoms first appeared when she was 3 years old and living in a Recreational Vehicle (RV) that had mold contamination in the HVAC system. About one year ago she discovered toxic mold contamination in the HVAC system of another RV where she lived. Her symptoms improved when she moved into a house. She had Congenital Hypertrophic Cardiomyopathy that required a heart transplant at age 3 months and is on Prograf for prevention of heart rejection.
A list of the patient’s symptoms before and after surgery is listed below in Table 1.
Table 1: Before and After Treatment Symptoms 0= No Symptoms To 10= Severe Symptoms
|
Symptoms |
Before Treatment |
After Treatment |
|
Fatigue |
8 |
2 |
|
Food Allergies |
3 |
0 |
|
Constipation |
5 |
5 |
|
Bloating/Gas |
4 |
4 |
|
Stomach Pain |
4 |
4 |
|
Gut Problems/Enteropathy |
1 |
1 |
|
Leaky Gut Syndrome |
1 |
1 |
|
Gluten Sensitivity |
2 |
2 |
|
Gastritis/Stomach Inflammation |
1 |
1 |
|
Colitis/Bowel Inflammation |
1 |
1 |
|
Hyperactivity |
9 |
9 |
|
Hypoglycemia/Low Blood Sugar |
5 |
5 |
|
Muscle/Joint Pain - Fibromyalgia |
8 |
3 |
|
Weakness |
8 |
3 |
|
Memory Loss |
8 |
2 |
|
Irritable Bowel Syndrome |
4 |
4 |
|
Insomnia |
8 |
2 |
|
Numbness/Tingling |
10 |
2 |
|
Anxiety, Depression, Irritability |
8 |
2 |
|
Skin Rashes |
9 |
0 |
|
Psoriasis |
7 |
0 |
|
Eczema |
9 |
0 |
|
Urticaria - Itching |
9 |
0 |
|
Shortness of Breath |
7 |
5 |
The patient’s January 20, 2020, environmental report from the RV she was living in for several months, showed very elevated levels of fungal spores in the air, which included a total of 9,880 mold spores per cubic meter of air with 7,100 Aspergillus/ Penicillium spores per cubic meter of air, as compared to only 208 spores per cubic meter of air outdoors (SEEML Labs, 203 Edinburgh Court, Greenville, SC 29607, 864-233-3770). There was visible mold behind the RV ceiling roofing in the HVAC ducting.
Sinus CT scan showed complete opacification of all eight sinuses and a fungus ball in the left maxillary sinus and bilateral turbinate hypertrophy. The endoscopic exam showed severe edema and erythema of all eight sinuses with panpolyposis and turbinate hypertrophy, gastroesophageal reflux disease, and Candida at base of tongue. Patient had high levels of ochratoxin A and mycophenolic acid before surgery while levels of ochratoxin A and mycophenolic acid were below detection limits following surgery (Table 2).
Table 2: Before and After Urine Mycotoxin Levels ppb= Parts per Billion.
|
Mycotoxin |
Before Surgery December 3, 2019 |
After Surgery December 23, 2021 |
Minimum Detection Limit |
|
Ochratoxin A |
102 ppb |
< 7.5 ppb |
7.5 ppb |
|
Mycophenolic Acid |
673.18 ppb |
<0.2 ppb |
0.2 ppb |
|
Citrinin |
< 25 ppb |
117.41 ppb |
37.4 |
Urine mycotoxin tests analyzed by Great Plains Lab, Overland, KS 66214.
The patient’s nose cultured Cladosporium, Microsporum, and Penicillium. She was placed on normal saline nasal irrigations with 5 drops of CitriDrops Dietary Supplement, which consists of 4 different citrus seed extracts with antimicrobial/antifungal properties, and Amphotericin-B nasal nebulization using a Rhino Clear Sprint nebulizer 2 mL BID. For mycotoxin detoxification, she used Oxygen 100% with face mask at 8 L/min, Acetyl Glutathione 300 mg BID, Opticleanse (a multifaceted supplement made by Xymogen, Orlando, FL, USA) for moderation of phase I liver detoxification and support of phase II liver detoxification pathways, and Intramax (another multifaceted supplement made by Drucker Labs in Plano, TX, USA), a multivitamin, mineral, and herbal formula bound to carbon to remove intracellular toxins. Surgery included standard FESS of all eight sinuses with irrigation of all eight sinuses with Amphotericin-B using a Cyclone (Stryker) Irrigator and a submucosal resection of the turbinates.
Please see Figure 1
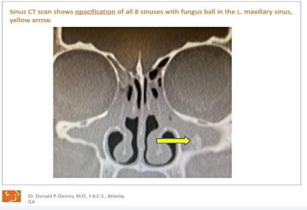
Figure 1: CT scan of 8 nasal sinuses.
for CT exam of 8 nasal sinuses and Figure 2
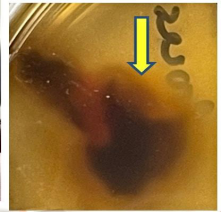
Figure 2: Ethmoid mucosa removed during sinus surgery with brown halo of mycotoxins coming out of ethmoid mucosal tissue.
for mycotoxin-containing exudate coming out of ethmoid mucosal tissue.
Chronic Fungal RhinoSinusitis (CFRS) is diagnosed by a number of means including: 1) nasal polyps, 2) allergic mucin, 3) computed tomography (CT) scans consistent with CRS (considered the Gold Standard of CRS Diagnosis, 4) a positive fungal culture or histology, and 5) type 1 hypersensitivity (Bent &Kuhn 1994). It is likely the patient has allergic fungal sinusitis due to fungus such as Candida, Cladosporium, Microsporum, and Penicillium being found on cultures, a fungus ball in the left maxillary sinus and having pan nasal polyposis No allergen testing was performed since the patient was on Prograf for to prevent heart transplant rejection.
The following videos may be of interest.
Video #1 Demonstrates Cyclone Amphotericin-B Irrigation
https://www.dropbox.com/s/gnos9lav2l4w8ej/Cyclone%20surgery%204-2-20.MOV?dl=0
Video #2 The Functions of the Cyclone Sinus Irrigator
https://www.dropbox.com/s/r97mtxvxr5vg0o4/Dr%20 Dennis%20Cyclone%20Entellus%202.mp4?dl=0
PROCEDURE
This patient had standard FESS surgery on all eight sinuses with generous sinusotomies on July 8, 2021. Frontal sinusotomies were done with either a balloon or standard FESS depending on degree of pathology. After FESS, all sinuses were irrigated with either Amphotericin-B (100 mg/L) or Voriconazole (412 mg/L) with the Cyclone (Stryker) sinus irrigation device using 2, 60 mL syringes for each sinus. All sinuses were irrigated beginning with frontal sinuses followed by maxillary, sphenoid, and ethmoid sinuses. All fluid was suctioned during irrigation to prevent recirculation of mycotoxins and MVOCs.
Patient returned on the sixth post-operative day, at which point essentially all of her dermatitis was resolved.
Figure 3

Figure 3: Legs pre and 6 days postoperatively.
Figure 4

Figure 4: Face before and 6 days after FESS with Amphotericin-BCyclone irrigation.
Figure 5

Figure 5: Hands and arms 6 days post op after FESS with Amphotericin-B Cyclone irrigation.
below show before and after pictures of the patient’s skin in the legs, face/neck, and hands/arms regions before and after initial fungal endoscopic treatment on July 8, 2021. Table 1 above notes that many of her health symptoms were largely resolved following treatment.
Patient had a recurrence of atopic dermatitis on November 4, 2021. A maxillary sinus surgery was done, and another fungus ball was removed from the left maxillary sinus as well as the left inferior turbinate and medial wall of the left maxillary sinus. Amphotericin-B irrigation was performed on 8 sinuses. Clearing of the facial atopic dermatitis occurred in hours post-surgery and clearing of the skin on her hands occurred in 4 days after surgery.
Another partial relapse occurred after dog exposure, and the patient had severe atopic dermatitis on the right hand. The patient was treated on November 18, 2021, with office endoscopic debridement and removal of fungus ball in left maxillary sinus and topical application of a mixture Amphotericin-B 2mL (3mg/30mL), Kenalog-40, 0.5 mL, and 2 mL of 1% Xylocaine with 1:100,000 Epinephrine.
A third partial relapse occurred, and the patient was treated again on December 7, 2021, with office endoscopic debridement and removal of fungus ball in left maxillary sinus and topical application of a mixture Amphotericin-B 2mL (3mg/30mL), Kenalog-40, 0.5 mL, and 2 mL of 1% Xylocaine with 1:100,000 Epinephrine.
Please see pictures of patient’s face and hands before and after endoscopic fungus removal in Figure 6
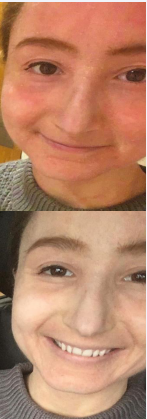
Figure 6: (After sinus surgery but with re-exposure to mold)Atopic dermatitis before and 4 hours after office endoscopic fungus removal and sinus injection of left maxillary sinus with Amphotericin-B, Kenalog-40, and 1% Xylocaine with 1:100,000 Epinephrine.
Figure 7

Figure 7: Atopic dermatitis of hand from fungus in left maxillary sinus before and 4 Days (December 7 and December 11, 2021) after office endoscopic removal of fungus with topical sinus injection of Amphotericin-B, Kenalog-40, and 1% Xylocaine with 1:100,000 Epinephrine.
DISCUSSION
This case study suggests that exposure to mold, mycotoxins, and MVOCs, either from the environment or by localized fungal sinus infections, can cause a wide range of health problems, including severe dermatitis, chronic fatigue, and neurological deficits. While large numbers of published studies have reported that exposure to indoor mold or moisture are associated with common allergic problems such as asthma and rhinitis [5,6] the relationships between mold and mycotoxins and other wideranging, chronic health problems are less well known.
Urine mycotoxin levels are helpful in discovering mycotoxins as a cause of multiple systemic symptoms. Several case reports have reported significant levels of mycotoxins in ethmoid sinus mucosa and in urine of humans exposed to toxic mold environments [18,19,26]. The patient’s urine showed elevated levels of 2 common mycotoxins on December 3, 2019, of 102 ppb Ochratoxin (Detection Limit<7.5 ppb) and 673.18 ppb mycophenolic acid (Detection Limit <0.2 ppb). After the first surgery on July 8, 2021, levels of ochratoxin and mycophenolic acid fell to below detection limits on December 23, 2021. An ochratoxin level of urine of 102 ppb is quite high; -a 2016 review of 23 worldwide studies involving a total of 2,115 subjects reported mean urine ochratoxin levels in the 23 groups of between 0.018 and 6.2 ppb [27]. Ochratoxin is produced by many Penicillium and Aspergillus species that are common on food and indoor air, including A. fumigatus, A. niger, A ochraceous, A. versicolor, P. crustosum, P. expansum, and P. verrucosum [16,28].
Mycophenolic acid is produced by a number of Penicillium species including common indoor species such as P. brevicompactum, P. roeufort, and P. verrucosum [16,28].
Perhaps the mycotoxins/allergens/volatile organics/ mold-contaminated indoor environment and the fungal ball colonization/infection caused the patient’s symptoms. An interesting Finnish study of 156 young adults with atopic dermatitis reported that skin symptoms were significantly worse in patients with both Candida skin sensitization and gastrointestinal Candida growth as compared to Candida skin sensitization without gastrointestinal growth [29].
Mechanism of Symptoms: Likely there are two or more genetic defects that are at play in about 20% of the population.
One is the immune reaction to mold itself, which is linked to AFS [30,31].We postulate the second may be inability to excrete the mycotoxins and MVOCs at a normal rate, which may be due to the MTHFR gene. The MTHFR gene would be involved by not allowing normal processing and excretion of the mycotoxins; there is some metabolic defect in the patients that does not allow them to excrete the toxins as rapidly as most people, and there is an allergic component to the mycotoxins and MVOCs.
Mycotoxins are microscopic solids that ride on dust particles and cause a long list of symptoms, and MVOCs are volatile chemicals that act like ether or glue fumes that enter the nose and can go directly into the brain to cause a number of neurological symptoms such as visual disturbance, hearing loss, dizziness, memory loss, concentration and comprehension problems, muscle weakness, paralysis, tremors, and immune suppression in decreasing IgG subclasses, as well as being carcinogenic. MVOCs can go through sheetrock and through a sealed plastic bag that will hold water, so when patients have severe neurological symptoms, it is best to get into a safe environment in which they know they are improving and deal with the remediation without entering the property. If after remediation the symptoms persist, it is best to relocate and not take anything from the contaminated place. Therefore, treatment first and most importantly is to get into an environment free of mold and mycotoxins, followed by saline irrigations with CitriDrops Dietary Supplement, a natural antimicrobial/antifungal, and Amphotericin-B nasal nebulization, mycotoxin detoxification with oxygen, which dilates the capillaries, Glutathione supplementation, Opticleanse, and Intramax. Removal of the antigen (mold, mycotoxins, and MVOCs) from the air and from the patient’s body are the most effective treatments for the immune reaction associated with toxin mold exposure. Elimination of the environmental exposure is paramount; without this, no other treatment is effective long term.
Testing for mold/mycotoxin/bacteria exposure, remediation of indoor environments, surgical treatment, and other medical/ nutritional interventions can be useful for diagnosing and treating a wide range of adverse health conditions including skin problems. If the mold-exposed patient is re-exposed to a lot of mycotoxins, they can experience a relapse, as our case study illustrates. To avoid relapse, it is helpful to avoid further mold exposure and, if exposed, to immediately treat with saline nasal irrigation and amphotericin sprays or nasal nebulization. For prevention of relapse in unfamiliar environments, Amphotericin nasal spray four times per day is helpful.
CONCLUSION
ENTs and other health care professionals need to more frequently consider mold and mycotoxin exposure as adverse health triggers. Questions about home/workplace environment, indoor environmental testing for molds, bacteria and water damage, SDA agar mold plate TAP testing on patient’s clothing (Immunolytics Lab),and urine mycotoxin tests (Real Time Lab/ Great Plains Lab) can be useful in determining and remediating environmental triggers. Many studies have reported that remediation of indoor mold and water damage can also significantly reduce rates of common allergic diseases such as rhinitis and asthma. A meta-analysis of 12 published studies reported that professional remediation of mold- and waterdamaged homes was associated with significant reductions both in wheezing (OR 0.64, 95% CI 0.55-0.75) and rhinitis symptoms
(OR 0.57, 95% CI 0.499-0.66) [32]. This study and several other studies have also reported that a multi-faceted treatment regime of endoscopic nasal surgery, environmental control, and medical/hormonal/nutritional treatment can potentially treat many health conditions, including chronic sinusitis, chronic fatigue, growth and thyroid hormone failure, neuropsychiatric problems, and dermatitis [9,26].
Much more research and clinical attention is needed to diagnose and treat the wide range of chronic health problems produced or aggravated by indoor mold, mycotoxins, MVOCs,bacteria, and moisture exposure.
ACKNOWLEDGEMENTS
We thank the patient for allowing us to report her case and present pictures of her and thank Carissa Gilman and Catherine Fruechtenicht for excellent editing. We also thank the many researchers we cite.
The most rapid resolution of symptoms and signs in the treatment of mold related illness is the removal of the antigen(s), fungus, mycotoxins, MVOC’s that are causing the immune reaction.
REFERENCES
- Bent JP 3rd, Kuhn FA. Diagnosis of allergic fungal sinusitis. Otolaryngol Head Neck Surg. 1994; 111: 580-8.
- Curtis L, Lieberman AD, Rea W, Stark M, Vetter M. Adverse human health effects of indoor molds. J Nutr Environ Med. 2004; 14: 261-74.
- Dooley M. MSW. A Comprehensive Review of Mold Research LiteratureFrom 2011-2018. Internal Medicine Review. 2020; 6: 1-39.
- Hope J. A review of the mechanism of injury and treatment approaches for illness resulting from exposure to water-damaged buildings, mold, and mycotoxins. ScientificWorldJournal. 2013; 2013: 767482.
- Quansah R, Jaakkola MS, Hugg TT, Heikkinen SA, Jaakkola JJ. Residential dampness and molds and the risk of developing asthma: a systematic review and meta-analysis. PLoS One. 2012; 7: e47526.
- Jaakkola MS, Quansah R, Hugg TT, Heikkinen SA, Jaakkola JJ. Association of indoor dampness and molds with rhinitis risk: a systematic review and meta-analysis. J Allergy Clin Immunol 2013; 132: 1099-1110.
- Ponikau JU, Sherris DA, Kern EB, Homburger HA, Frigas E, Gaffey TA, Roberts GD. The diagnosis and incidence of allergic fungal sinusitis. Mayo Clin Proc. 1999; 74: 877-84.
- Brewer JH, Thrasher JD, Straus DC, Madison RA, Hooper D. Detection of mycotoxins in patients with chronic fatigue syndrome. Toxins. 2013; 5: 605-17.
- Dennis D, Robertson D, Curtis L, Black J. Fungal exposure endocrinopathy in sinusitis with growth hormone deficiency: Dennis- Robertson syndrome. Toxicol Ind Health. 2009; 25: 669-80.
- Hyvonen S, Poussa T, Lohi J, Tuuminen T. High prevalence of neurological sequelae and multiple chemical sensitivity among occupants of a Finnish police station damaged by dampness microbiota. Arch Environ Occup Health. 2021; 76: 145-151.
- Hyvonen S, Syrjala H. Asthma Case Cluster during Renovation of aWater-Damaged and Toxic Building. Microorganisms. 2019; 7: 642.
- Zhang X, Norback D, Fan Q, Bai X, Li T, Zhang Y, et al. Dampness and mold in homes across China: Associations with rhinitis, ocular, throat and dermal symptoms, headache and fatigue among adults. Indoor Air. 2019; 29: 30-42.
- Hyvonen S, Lohi J, Tuuminen T. Moist and Mold Exposure is Associated With High Prevalence of Neurological Symptoms and MCS in a Finnish Hospital Workers Cohort. Saf Health Work. 2020; 11: 173-177.
- Hyvonen SM, Lohi JJ, Rasanen LA, Heinonen T, Mannerstrom M, Vaali K, et al. Association of toxic indoor air with multi-organ symptoms in pupils attending a moisture-damaged school in Finland. Am J Clin Exp Immunol. 2020; 9: 101-113.
- Kilburn KH. Neurobehavioral and pulmonary impairment in 105 adults with indoor exposure to molds compared to 100 exposed to chemicals. Toxicol Ind Health. 2009; 25: 681-92.
- Brase S, Encinas A, Keck J, Nising CF. Chemistry and biology of mycotoxins and related fungal metabolites. Chem Rev. 2009; 109: 3903-90.
- Hooper DG, Bolton VE, Guilford FT, Straus DC. Mycotoxin detection in human samples from patients exposed to environmental molds. Int J Mol Sci. 2009; 10: 1465-75.
- Dennis D, Thrasher J. Nasal Fungal Pathology and Trichothcenes Associated with Water-Damaged School and House. Austin Journal of Otolaryngology. 2016; 3: 1072.
- Dennis D, Thrasher J. Surgical and medical managment of sinus mucosal and systematic mycotoxicosis. Otolaryngol Reconstructive Surgery. 2017; 3: 117.
- Celakovska J, Vankova R, Bukac J, Cermakova E, Andrys C, KrejsekJ. Atopic Dermatitis and Sensitisation to Molecular Components of Alternaria, Cladosporium, Penicillium, Aspergillus, and Malassezia- Results of Allergy Explorer ALEX 2. J Fungi (Basel). 2021; 7: 183.
- Tan RA, Corren J. The relationship of rhinitis and asthma, sinusitis, food allergy, and eczema. Immunol Allergy Clin North Am. 2011; 31: 481-91.
- Chang EH, Stern DA, Willis AL, Guerra S, Wright AL, Martinez FD. Early life risk factors for chronic sinusitis: A longitudinal birth cohort study. J Allergy Clin Immunol. 2018; 141: 1291-1297.
- Bornehag CG, Sundell J, Hagerhed-Engman L, Sigsggard T, Janson S, Aberg N. ‘Dampness’ at home and its association with airway, nose, and skin symptoms among 10,851 preschool children in Sweden: a cross-sectional study. Indoor Air. 2005; 15: 48-55.
- Shi H, Wan G, Wang T, Zhu J, Jiang L, Ma S, et al. Prevalence and influencing risk factors of eczema among preschool children in Urumqi city: a cross-sectional survey. BMC Paediatrics. 2021; 21: 347.
- Seo S, Han Y, Kim J, Choung JT, Kim BJ, Ahn K. Infrared camera-proven water-damaged homes are associated with the severity of atopic dermatitis in children. Ann Allergy Asthma Immunol. 2014; 113: 549- 55.
- Dennis D, Curtis L, Phares J. Surgical and Medical Management of Mycotoxin Neurotoxicity and Neuropsychological Symptoms via Endoscopic Sinusotomies and Cyclone Antifungal Irrigation. Ann Otolaryngol Rhinol. 2021; 8: 1259.
- Fromme H, Gareis M, Volkel W, Gottschalk C. Overall internal exposure to mycotoxins and their occurrence in occupational and residential settings--An overview. Int J Hyg Environ Health. 2016; 219: 143-65.
- Samson RA HJ, Thrane U, Frisvad JC, Andersen B. Food and Indoor Fungi. CBS- KNAW Fungal Biodiversity Centre, Utecht, The Netherlands. 2010.
- Savolainen J, Lammintausta K, Kalimo K, Viander M. Candida albicans and atopic dermatitis. Clin Exp Allergy. 1993; 23: 332-9.
- Kotzin BL, Leung DY, Kappler J, Marrack P. Superantigens and their potential role in human disease. Adv Immunol. 1993; 54: 99-166.
- Schubert MS. A superantigen hypothesis for the pathogenesis of chronic hypertrophic rhinosinusitis, allergic fungal sinusitis, and related disorders. Ann Allergy Asthma Immunol. 2001; 87: 181-8.
- Sauni R, Verbeek JH, Uitti J, Jauhiainen M, Kreiss K, Sigsgaard T. Remediating buildings damaged by dampness and mould for preventing or reducing respiratory tract symptoms, infections and asthma. Cochrane Database Syst Rev. 2011; CD007897.









































































































































