Contemporary Diagnostic of Nasal Obstruction - Basic Errors and How to Avoid Them
- 1. Faculty of Medicine, University of Latvia, Germany
- 2. Department of Otorhinolaryngology, Head and Neck Surgery, Paracelsus Medical University, Austria
ABSTRACT
Missing success in rhinosurgery or conservative treatment of nasal obstruction can be caused by insufficient or erroneous diagnostic. The review follows recent critical analyses of test methods for nasal obstruction by scientists and rhinologists and describes new ways as to the state of art in science and technique. 4-Phase-Rhinomanometry (4PR) with logarithmic parameters is the basic method to determine the degree of obstruction and to classify it. The detailed morphologic analysis can be carried out by Computational Fluid Dynamics (CFD) or transferring radiological DICOM-data into stereolithography- files and generating 3D-printed models. A preoperative simulation of surgical steps can be carried out by both methods.
Following Weber-Fechner´s basic law of psychophysics a correlation between the feeling of obstruction and rhinomanometric results can be achieved only by applicating logarithmic parameters.
The nose is a Starling-resistor and the quantitative determination of the nasal valve activity is mandatory. It is possible by the evaluation of loops in 4PR-diagrams. More precise methods are under development.
The morphology and function of the nasal airway has to be included in the diagnosis of sleep disordered breathing. The influence of the body position can be determined and the effectivity of nCPAP-treatment or surgery predicted.
Simplified methods as PNIF should be refused because of missing consideration of the nasal valve elasticity.
Subjective scores (NOSE-score, SNOT-score) have a limited meaningfulness in rhinological diseases, where obstruction determines the severity. The feeling of obstruction is better described by Visual-analogue-scales (VAS) recorded together with 4PR-measurements.
KEYWORDS
- Nasal obstruction; objective measurement; 4-phase-rhinomanometry; Computational fluid dynamics; 3D-printing
CITATION
Vogt K, Roesch S, Bauer SM, Neumaier P (2022) Contemporary Diagnostic of Nasal Obstruction - Basic Errors and How to Avoid Them Ann Otolaryngol Rhinol 9(4): 1297.
ABBREVIATIONS
4PR: 4-phase-rhinomanometry; CFD: Computational Fluid Dynamics; PNIF: Peak Nasal Inspiratory Flow; VAS: Visual- analogue scale; STL: Stereolithography; ISCOANA: International Standard Committee on the Objective Assessment of the Nasal Airway; HPC: High Performance Computing; AI: Artificial Intelligence; DVT: Digital Volume Tomography; CT: Cone Beam Tomography; Reff: Effective Resistance; LReff: Logarithmic Effective Resistance; VR: Vertex resistance; LVR: Logarithmic Vertex Resistance.
INTRODUCTION
Under the contemporary conditions including endoscopic and radiologic methods it seems to be simple to find a correct diagnosis and adequate indications for the treatment of rhinologic diseases. This statement is correct as long as obstruction is not the only one symptom determining the indications and extend of restoration of the nasal breathing function, in particular of irreversible surgical steps. The diagnosis of nasal obstruction is a matter of contrary discussion for more than 100 years by surgeons and scientist, but the general state of art in technique and informatics was and is frequently not implemented there. Missing objective and subjective success in nasal surgery with personal, social and also financial consequences as reported between 30 and 50% worldwide is at least to some extend a follow-up of incomplete or erroneous diagnostic.
Diagnostic measures in an institution or clinic usually depend on opinions learned from textbooks, the usual order of procedures in the institution, the available technical equipment or the personal experience of the practicing surgeon or his team, sometimes also on legal prescriptions. The introduction of updates or improvements for traditional methods or new techniques is long lasting and sometimes a controversial discussion. The reasons are mostly difficulties to understand the scientific or technical background. The functional diagnostic of nasal obstruction is a typical example with many disastrous consequences.
Vice versa, standards created by responsible scientists of different fields and medical professionals can be very helpful. The “International Standardization Committee on the Objective Assessment of the Nasal Airway” (ISCOANA), an organ of the International Rhinologic Society IRS, created a standard in 1984 [1], but did not update it for a very long time. Only in 2016, during an international meeting of specialists at the University of Latvia in Riga, was the validity of nasal function tests extensively discussed and a new standard created and published [2]. Following that, a group of Austrian and German researchers in physics, informatics, medical techniques and experienced rhinologists started the research project “Rhinodiagnost” (www. rhinodiagnost.eu) supported by their governments. Essential results with practical relevance are implemented here.
DEFINITION OF NASAL OBSTRUCTION
Nasal obstruction or resistance is the relation between the narino-choanal differential pressure ?P and the intranasal volume stream V?
It depends on the three-dimensional configuration of the nasal breathing channel. The key to a successful treatment is the determination of the degree of obstruction followed by a precise analysis of the anatomical structures causing it. The nasal cavity is an irregular flow body, which can be compared with a “tube” or a “diaphragm”. With an acceptable appropriation the basic law of HAGEN-POISEUILLE was formerly applied, which means that the nasal airway resistance is primarily depending on the 4th power of the diameter and only in a minor extend on the length of the channel.
with the resistance R, the viscosity of air η, the length l and the radius r. A very small reduction of the diameter or cross-sectional area has a big effect on the nasal resistance.
Within the experimental part of the Rhinodiagnost-project the relation between resistance, radius and length was tested by a special simulator. Contemporary step motors and linear actuators can be used to set up precisely working pumps which are digitally controlled. These techniques are integrated in the „Artificial Noses“ ARNO 4 and ARNO 5 (Figure 1).
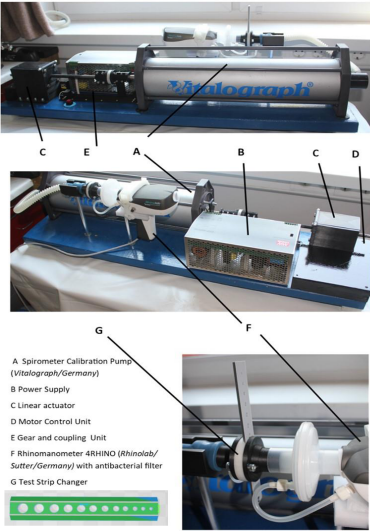
Figure 1: Breathing simulator ARNO 5 (MedTecResearch/Germany) and orifice strip.
By these simulators it is not only possible to simulate breathing through different models but also to check the precision of different rhinomanometers. As an example, Figure 2
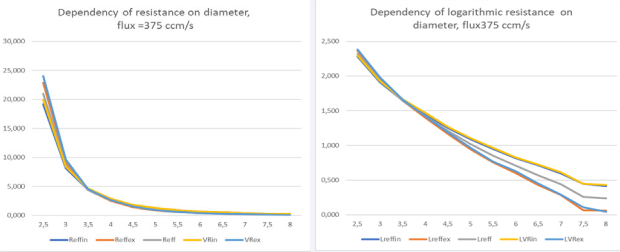
Figure 2: Dependency of linear and logarithmic resistances on the diameter of orifices.
shows the relation between the width of holes and linear and logarithmic resistances as parameters of 4-phase-rhinomanometry. The range of simulated resistances in holes corresponds with the total range of resistances as measured in non-obstructed and obstructed nasal sides during nasal breathing. For flows through orifices as shown in Figure 1, the exponential decrease of resistances with increasing orifice diameter do is more precise described by the following formula
with : orifice diameter;
: pipe diameter; ρ: density;
: volume flux;
: coefficient of discharge. The simulations also have shown the minor influence of length on resistance.
The consequences following the confirmed background theoretical for the clinical practice are:
• The human eye cannot estimate the degree of nasal obstruction because the resistance depends exponentially on the diameter.
• The inspection of the nose by speculum or endoscope can identify airway restrictions in the anterior part but sometimes not in subsequent areas.
• A functional diagnosis and detailed morphologic analysis of the airflow in obstruction before treatment is mandatory for precision diagnosis.
• Differential pressure and flow are the key parameters to describe the nasal resistance and to understand the clinical phenomenon of nasal obstruction.
4-phase-rhinomanometry (4PR) as basement of functional diagnosis
The history of “classic” rhinomanometry and similar methods is longer than 100 years. A new era started around 1980 by introducing digital measurement methods replacing the graphical evaluation of curves before. The first computer aided rhinomanometer was introduced in 1990 [3]. The numeric evaluation followed first the old graphical standard with the determination of flow in 150 Pa or the “ BROMS´method” in Scandinavia. The transition to digital methods showed us soon, that there have been 3 main reasons for leaving the one-pointmeasurements behind us:
1. Resistances at different pressure or flow levels are not identical
2. The calculation of a linear resistance in accelerating or decelerating air stream is mathematic nonsense
3. Many patients cannot reach a pressure level at 150 Pa
The solution of the problem was possible by computerized rhinomanometry, which is for more than 30 years the “golden standard”. Breathing waves follow the same rules as electromagnetic waves. They are simply slower and asymmetric. Thus, we can apply the physics and laws of electro-engineering. The voltage of 230 V as measured daily in power stations or in the sockets of every household is the “Effective Voltage” or in English RMS (root mean square) and the power intensity is the “Effective Intensity”. These parameters have been introduced by us in 1994 within the context of “High Resolution Rhinomanometry”, which was later due to the ISCOANA renamed as “4-phaserhinomanometry” [4].
Figure 3
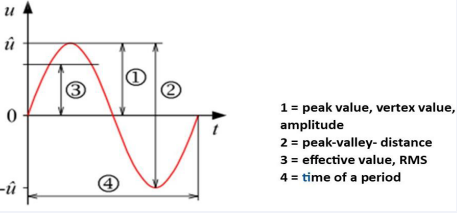
Figure 3: Parameters of voltage in an electric sinus – wave.
explains that we are dealing when measuring parameters of the nasal air stream with very similar processes as in electro engineering.
In statistics, the root mean square (abbreviated RMS or rms), also known as the quadratic mean, is a statistical measure defined as the square root of the arithmetic mean of the squares of a set of numbers. It is of outstanding importance that this value can be calculated also for a continuously varying function as in breathing waves. The air stream can be steady or unsteady, laminar or turbulent.
In the case of a set of n values x1 , x2 , …, xn, RMS can be calculated as
In the practice of 4PR we calculate the RMS for pressure and flow from all measured values during the data acquisition process and obtain in this way correct measured values instead of weak estimations.
Finally, there are 2 measurable and reliable parameters, which inform us about the energetics of the nasal air stream: Effective Resistance Reff and Vertex Resistance VR. The effective resistance can be measured through the entire breath, in inspiration or expiration, vertex resistance at the top of the breathing wave in inspiration and expiration.
For the clinical diagnostic Reff and VR are transformed into logarithmic values as LReff, LReffin, LReffex, LVRin and LVRex. Because small and negative numbers are difficult to handle, we introduced the logarithm of the 10-fold value as basement for the classification of the nasal obstruction. The ISCOANA followed the proposal.
For example
LReffIn = log(10*ReffIn)
The introduction of logarithmic resistance values into the clinical practice is one of the most important advantages of 4-phase-rhinomanometry.
4PR and psychophysics of breathing
During the last years it was a big matter of international discussion with controversial results, if rhinomanometric measurements or results of other nasal function tests are related to the subjective sensing of obstruction. Nearly all of the cited authors concluded that a statistically significant correlation between objective results and sensing of obstruction does seemingly not exist. However, the reasons for the missing relation have not really been interpreted but are quite clear: only non-logarithmic parameters have been considered.
In psychophysics, the Weber–Fechner law combines two different laws of human perception. Ernst Heinrich Weber (1795–1878) was one of the first to approach the study of the human response to a physical stimulus in a quantitative fashion. Weber found that the just noticeable difference (jnd) between two weights was approximately proportional to the weights. Thus, if the weight of 105 g can (only just) be distinguished from that of 100 g, the jnd (or differential threshold) is 5 g. If the mass is doubled, the differential threshold also doubles to 10 g, so that 210 g can be distinguished from 200 g. In this example, a weight (any weight) seems to have to increase by 5% for someone to be able to reliably detect the increase, and this minimum required fractional increase (of 5/100 of the original weight) is referred to as the “Weber fraction” for detecting changes in weight. Gustav Theodor Fechner (1801–1887), a scholar of Weber, later used Weber’s findings to construct a psychophysical scale in which he described the relationship between the physical magnitude of a stimulus and its (subjectively) perceived intensity. Fechner’s law (better referred to as Fechner’s scale) states that subjective sensation is proportional to the logarithm of the stimulus intensity. Fechner´s scaling has been mathematically formalized.
Otorhinolaryngologists know the logarithmic dB-scale in acoustics, it is well known for smelling but was never applied to determine the relation between nasal airway resistance and the feeling of obstruction. The sensing of obstruction is merging the feeling of increased power to breath with the feeling of the temperature gradient and may be also the wall sheer stress of the airstream. The additional documentation on a VAS-scale creates reliable data for the feeling of impaired breathing at the measured side in this moment.
In a comprehensive multicentric study with 36,500 measurements [5] we could find a statistically significant relation between the logarithmic effective resistances and data obtained from a VAS scale. It confirms the importance to consider objective and subjective results together, in particular when comparing pre- and postoperative results.
4PR and the nasal valve
The usual standardized graphic in rhinomanometry is an xydiagram with the differential pressure on the y-axis and the flow on the x-axis (Figure 4).
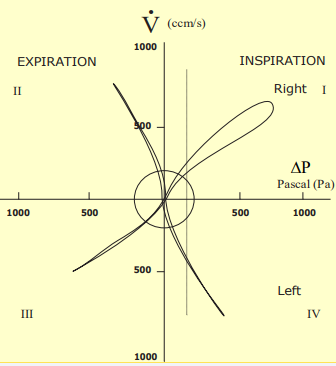
Figure 4: Standard xy-diagram of 4-phase-rhinomanometry.
Principally, the pressure-flow relation of the nasal airstream can also be depicted on 2 channels of an xt-diagram (Figure 5),
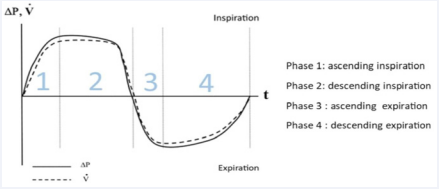
Figure 5: Time relation of differential pressure and flow.
where the 4 breathing phases can be clearly identified.
After the introduction of digital rhinomanometers and the recording of complete breaths sometimes loops in the standard diagram have been recorded during inspiration, which have been formerly considered as hysteresis due to different inertia of the pressure and flow sensors. That was excluded by the application of mass flow sensors for the flux, but inspiratory loops still have been observed in about 25% of all measurements. The curve type with expressed inspiratory loops (Figure 4, right side) was named the elastic type [4]. The time dependent course of pressure and flow in such cases are shown in Figure 6.
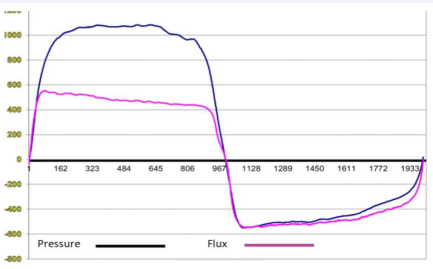
Figure 6: Timeline of intranasal pressure and flow in valve effects.
The flow-curve follows the pressure curve in inspiration up to a level of about 580 Pa and in the descending phase downwards from 400 Pa, while in expiration both curves are following each other. The ascending inspiratory flow releases the Bernouilli-effect by generating a negative pressure in the valve area and moves the lateral nasal wall inside. The reduction of the cross-sectional area causes the temporary increase of the resistance and keeps the flow on the same level until the pressure goes down. Inspiratory loops are an additional diagnostic information indicating a valve effect, which can be achieved only when the 4 phases of breathing are separately analysed.
The special morphology of the nasal valve, its dimensions and mobility are an extraordinary importance in every rhinomanometric measurement. Failures in all measurements occur if the pressure tube is fixed in the nose by preformed plugs instead by mobile tape. The role of the nasal valve can also be verified with 4PR by tape retraction tests (Cottle-test) or spreader devices to investigate their efficacy [3]. A detailed description for the quantitative evaluation of the “inspiratory loop area” of 4PR and respective statistic data were recently, for the first time, published by Gagnieur et al. [6].
Quantitative methods to determine the valve movement in dependency of breathing by strain gauge measurements as introduced In 2018 by Akmenkalne et al.[7] clearly showed, that the deflection starts already in quiet breathing. Therefore, techniques for its easy visualizing “elastography” are under development. Also, the mechanical properties as for instance the Elasticity Module E could be determined by “elastometry” using a special measurement forceps, by which we could find first clinical results.
Comparability and classification of 4PR
After the introduction of effective values and their logarithmic transformations it was mandatory to create a classification for the severity of obstruction. That was done in 2 multicentric studies of 36,563 unilateral measurements with decongestion tests and 10,033 measurements of the total nasal resistance [5,8] (Table 1).
Table 1: Clinical classification of Logarithmic Effective Resistance (LReff).
|
|
Unilateral Logarithmic Effective Resistance (LReff) |
Calculated bilateral Logarithmic Effective Resistance (LReff) |
|||
|
class |
untreated |
after decongestion |
untreated |
after decongestion |
|
|
1 |
0–19% |
< 0.71 |
< 0.63 |
< 0.42 |
< 0.36 |
|
2 |
20–39% |
0.71–0.89 |
0.63–0.78 |
0.42 - 0.57 |
0.36 - 0.47 |
|
3 |
40–59% |
0.89–1.08 |
0.78–0.94 |
0.57 - 0.70 |
0.48 - 0.59 |
|
4 |
60–79% |
1.09–1.35 |
0.94–1.18 |
0.70 - 0.90 |
0.59 - 0.76 |
|
5 |
80–100% |
> 1.35 |
> 1.18 |
> 0.90 |
> 0.76 |
The classification is also valid for LReffIn, LReffex, LVRin and LVRex in adults of the Caucasian race and is applied in 8 European and Asian countries, Canada and in the USA. A comparative study in China showed only minor differences for the Chinese population. Peksis et al., investigated the age dependency in kids and teenagers and published correction factors for that group [9]
The classifications above are obtained from measurements in rest and upright sitting position. The second measurement in decongestion tests was carried out 10 min after application of xylometazoline spray 0.1%.
Nasal obstruction and sleep disordered breathing
The relations between nasal obstruction and sleep disordered breathing (SDB) or obstructive sleep apnoea are unquestionable. After the introduction of 4 PR, one of the pioneers of diagnosis and therapy of SDB, Christian Guilleminaut and his co-workers [10], tested it in a clinical study and recommended as well the measurement method as the new logarithmic parameters within this framework. That was followed by numerous other studies [11,12]. In addition to generally testing the nasal obstruction as part of the entire respiration system, the influence of body position is of high importance: changing from supine to inclined position can improve the nasal resistance about 1 class. The compatibility of nCPAP-devices is dependent upon an appropriate nasal conductivity. Widening the nasal entrance by spreader devices can be tested.
Refinement of the morphological analysis of obstruction
Radiological diagnostic as CT, MRI or cone beam tomography can provide us with excellent information about the anatomy of the nose, the paranasal sinuses and other adjacent structures, but it cannot inform us about the geometry of the nasal air stream and the changes in different places of interest. Computational Fluid Dynamics (CFD) cannot only visualize the airstream but also calculate the variations of pressure and flow as well as the temperature gradient under different flow conditions at regions of interest. CFD is the key to modern aerodynamics and is included into the construction of techniques, where an airstream or fluid stream plays an important role as in airplanes or big tube systems. The concept of 4-Phase-Rhinomanometry was confirmed by CFD already in 2009[4].
An example of how CFD simulations can extend standard rhinological diagnostics is given in Figure 7.
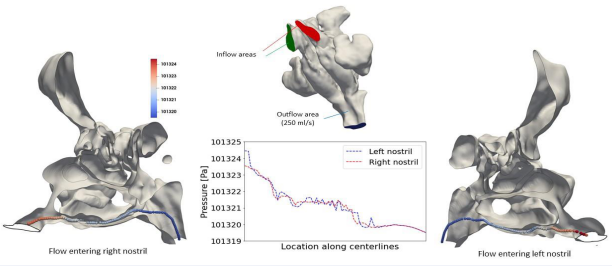
Figure 7: CFD-analysis: area-averaged pressure (M.Ruettgers).
It shows the pressure distribution along geometric centerlines in the left and right nasal cavity. The general concept and the numerical method employed for the simulation and visualization of the pressure loss inside the nasal cavity are explained in detail in [13,14].
In [15], these methods were further extended to allow surgeons to evaluate a planned surgery virtually using CFD simulations. However, the introduction of CFD as a routine method still needs the generation and testing of standard procedures by rhinologists and IT experts as well as access to High-Performance Computing (HPC) systems. On this account, the possibility of using Artificial Intelligence (AI) to accelerate the simulations is under investigation in current studies.
Besides complex simulations of respiration, the generation of 3D models of the nasal cavity from DICOM-data of CT, DVT, or MRI can also support physicians in their decision-making. The resulting stereolithography (STL) files can for example be used to print 3D models of the nose and adjacent structures. For the conversion of the DICOM files, AI algorithms can be used as well as open-source programs available on the internet (“Invesalius”). The STL files can be easily opened by different open-source programs such as MS Windows “3D-Builder” (Figure 8).
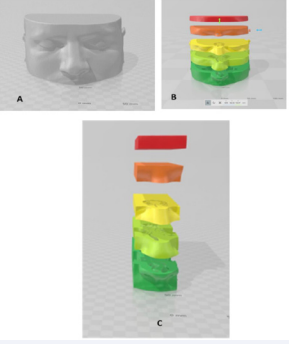
Figure 8: Preparing of a 3D-print from DICOM-data.
The model of the complete head (A) has to be divided into 4 to 6 layers (B) and the regions of interest are chosen. Additional information about the axial construction of the nasal cavity and sinuses can be achieved already by this step. By lateral vertical cuts, the model gets reduced (C) to save time and material for printing.
It follows the “slicing” process which is the transfer of the stereolithography-data as to the specific requirements of the printer and the used filament and the printing process. Figure 9
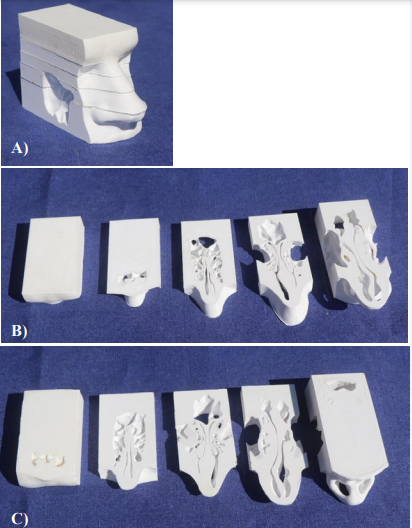
Figure 9: Reassembled model A and 5 different layers from cranial (B) and caudal(C) side.
shows the re-assembled 3D-model and the printed layers in cranial and caudal view.
The assembled models can now be encased in an adaptable box, and via this box, connected to a rhinomanometer and a tube for breathing or a ventilator. After the unilateral or total resistances of the model are measured, stepwise virtual surgery can follow and the measurements can be repeated to estimate the results of detailed surgical steps figure 10.

Figure 10: Encased model for rhinomanometric measurement with rhinomanometer 4PR2.
We may recommend 3D-printing of nasal models and the resistance-controlled simulation of surgery in difficult cases with a high degree of obstruction as well as for beginners in nasal surgery. The additional information we could get up to now was unexpected even for experienced rhinosurgeons. 3D-printers More popular is the “Acoustic Rhinometry”. It measures the cross-sectional area at the nasal entrance, but the results deliver no information about the energetics of the nasal air stream. Therefore, it is not used in Germany or Austria in the daily routine.
The measurement of Peak Nasal Inspiratory Flow (PNIF) is a simple measurement, wide spread in the world, but unfortunately not acceptable. It is not considering the essential influence of the elastic deformation of the nasal wing in maximal inspiration.
SUMMARY AND RECOMMENDATIONS FOR THE DIAGNOSIS OF NASAL OBSTRUCTION
• The human eye cannot estimate the degree of nasal obstruction because the resistance depends exponentially on the diameter and in a minor extent on the length of a constricted area. Therefore, the objective measurement of obstruction by physically correct and technically reliable methods is mandatory. Logarithmic parameters are classified and recommended within the last ISCOANA – standard.
• The sensation of airway resistance is following WeberFechner´s law and depends logarithmically on the aerodynamic resistance of the nasal airway. It should be recorded on a VAS-scale for every side together with the rhinomanometric measurement.
• The nose is not a rigid anatomic structure but a Starlingresistor, which means that the resistance is increasing with the air flux because of the influence of elasticity of the lateral nasal wall. Semi-quantitative information is given by the inspiratory loop area in 4 PR. More precise methods for the determination of the elasticity of the lateral nasal wall are under development.
• The nasal valve is ONE physiological unit consisting of different anatomic compartments. The differentiation between “external valve ” and “internal valve” is not corresponding with the real physiology and is therefore misleading.
• The diagnosis of sleep disordered breathing should always include the quantitative evaluation of nasal obstruction.
• Score systems as “NOSE-score” or “SNOT-score” have only a limited value for the indication and success control of nasal surgery because of incorrect relations with the feeling of obstruction. The outcome of questionnaires is sometimes influenced by biases.
ACKNOWLEDGEMENTS
The authors wish to thank Mario Ruettgers and Moritz Waldmann as well as Prof. Wolfgang Schroeder, director of the Institute of Aerodynamics, RWTH Aachen University, and the co-workers of the Supercomputing Center Jülich /Germany for their permanent cooperation in developing advanced diagnostic methods in rhinology and to introduce them in the practice.
REFERENCES
- Clement PA, Gordts F. Consensus report on acoustic rhinometry and rhinomanometry. Rhinology. 2005; 43: 169-179.
- Vogt K,Bachmann-Harildstad G,Lintermann A, Nechyporenko A, Peters F, Wernecke KD, et al. The new agreement of the International RIGA Consensus conference on nasal airway function tests. Rhinology. 2018; 56: 1-11.
- Vogt K, Wernecke KD, Sachse D, Kriesmer Th. Computergestütztes System zur rhinologischen Funktionsdiagnostik HNO. 1990; 38: 110-115.
- Vogt K, Jalowayski A, Althaus W, Cao C, Han D, Hasse W, et al. Basic and practice of 4-phase-rhinomanoetry 2010. Rhinol Suppl. 2010; 21:1-48.
- Vogt K, Wernecke KD, Behrbohm H, Gubisch W, Argale M. Four-phase rhinomanometry: a multicentric retrospective analysis of 36,563 clinical measurements. Eur Arch OtoRhinoLaryngol. 2016; 273: 1185-1198.
- Gagnieur P, Fieux M, Louis B. Objective diagnosis of internal nasal valve collapse by four-phase-rhinomanometry. Laryngoscope Investig Otolaryngol. 2022: 7: 388-394.
- Akmenkalne L, Prill M, Vogt K. Nasal valve elastographyquatitative determination of the mobility of the nasal valve. Rhinology Online. 2019; 2: 81-86.
- Vogt K, Wernecke K-D, Argale M, Kaulina K. Classification of total nasal obstruction in 10,033 cases by 4-phase –rhinomanometry. Romanian J Rhinology. 2016; 6: 149-160.
- Peksis K, Unger J, Paulauska S, Emsina1 A, Blumbergs M, Vogt K, et al. Relationships among nasal resistance, age and anthropometric parameters of the nose during growth. Rhinology Online. 2018; 1: 112-121.
- Toh ST, Lin CH, Guilleminault C. Usage of four-phase high-resolution rhinomanometry and measurement of nasal resistance in sleep- disordered breathing. The Laryngoscope. 2012; 122: 2343-2349.
- Lofaso A, Coste M, Ortho PD. Nasal obstruction as a risk factor for sleep apnoea syndrome. European Respiratory J. 2012; 16: 639-643.
- Sunderram J, Ayappa I, Rapoport D. PAP Adherence and NasalResistance. A Randomized Controlled Trial of CPAP flex versus CPAPin World Trade Center Responders. Ann Am Thoracic Soc. 2021; 18: 668-677.
- Waldmann M, Grosch A, Witzler C, Vogt K, Kohn C, Schröder W, et al. An effective simulation- and measurement-based workflow for enhanced diagnostics in rhinology. Med Biol Eng Comput. 2022; 60: 365-391.
- Rüttgers M, Waldmann M, Schroeder W, Lintermann A. Machine-Learning-Based Control of Perturbed and Heated Channel Flows, in Jagode H, Anzt H, Ltaief H, and Luszczek P (Editors) “High Performance Computing. Springer International Publishing, 2021; 7-22.
- Waldmann M, Rüttgers M, Lintermann A, Schröder W. Virtual Surgeries of Nasal Cavities Using a Coupled Lattice-Boltzmann–Level- Set Approach. J Engineering Sci Med Diagn Therapy. 2022; 5.









































































































































