Locally Advanced Nasopharyngeal Carcinoma Complicated with Secondary Tuberculosis: A Case Report
- 1. Department of Radiation Oncology, Shenzhen People’s Hospital (The Second Clinical Medical College, Jinan University; The First Affiliated Hospital, Southern University of Science and Technology), China
- 2. Department of Radiation Oncology, The Third Affiliated Hospital of Shenzhen University (Shenzhen Luohu People’s Hospital), People’s Republic of China #These authors contributed equally to this work
ABSTRACT
Background: The treatment regimen, adverse drug reactions, and prognosis of nasopharyngeal carcinoma complicated with secondary pulmonary tuberculosis have been controversial.
Case presentation: We report a rare case of advanced nasopharyngeal carcinoma complicated with secondary pulmonary tuberculosis. Considering the late stage of nasopharyngeal carcinoma, three cycles of induction chemotherapy was followed by concurrent radiotherapy and chemotherapy. Secondary pulmonary tuberculosis was found on chest CT during the treatment of nasopharyngeal carcinoma and a 2HRtE / 7HRt regimen was used for treatment. The patient showed complete response to the treatment of nasopharyngeal carcinoma without recurrence or metastasis, and pulmonary tuberculosis was well controlled.
Conclusion: The treatment of advanced nasopharyngeal carcinoma complicated with secondary pulmonary tuberculosis is challenging, and there have been few relevant reports in the literature. Through a well-designed multimodal treatment scheme, patients are expected to survive for many years and the quality of life of the patients is guaranteed.
KEYWORDS
- Nasopharyngeal carcinoma
- Secondary pulmonary tuberculosis
- Treatment plan
- Radiotherapy
- Chemotherapy
CITATION
Liang-Chen X, Han L, Wen-Yi L, Fang-Zheng Z, Shi-Hai W (2022) Locally Advanced Nasopharyngeal Carcinoma Complicated with Secondary Tuberculosis: A Case Report. Ann Otolaryngol Rhinol 9(1): 1282.
ABBREVIATIONS
CT: Computed Tomography; TPF: Paclitaxel, Lobaplatin, 5-fu; H: Isoniazid; Rt: Rifampicin Derivative; E: Ethambutol
INTRODUCTION
Nasopharyngeal carcinoma or secondary tuberculosis that occurs alone is a common clinical disease and frequently- occurring disease [1]. There are many reports on lung cancer complicated with pulmonary tuberculosis in the clinic, but nasopharyngeal carcinoma complicated with secondary pulmonary tuberculosis is rare. Once diagnosed, it is necessary to strictly design multimodal treatment schemes that include surgery, radiotherapy, chemotherapy, and anti-tuberculosis treatment. The real challenge is whether multiple drugs will have cross effects and increase the toxic and side effects in the body. The present paper reports a case of nasopharyngeal squamous cell carcinoma complicated with secondary pulmonary tuberculosis to improve the treatment of patients diagnosed with these diseases.
CASE PRESENTATION
First admission
The first admission time was 14:00 on January 10, 2020.
Chief complaints
A 40-year-old male patient was admitted to the hospital five days after he found a mass in the right nasopharynx due to frequent intermittent bleeding for five months in the right nasal cavity.
History of present illness
Nosebleeds experienced by the patient were exacerbated with the passage of time. The patient recently (within 20 days) developed diplopia in the right eye with right facial numbness. The patient had no fever, headache, chest tightness, or shortness of breath.
History of past illness
The patient had no history of past illness and was in good health. The patient had no history of smoking or drinking.
Personal and family history
No relevant personal or family history was found.
Physical examination
An enlarged lymph node of approximately 4 cm × 3 cm was palpated in the left upper neck. An enlarged lymph node approximately 3 cm × 2 cm was palpated in the right upper neck. The enlarged lymph nodes had no tenderness, the texture was slightly hard, and additional superficial lymph nodes are not palpable. Bilateral nasal cavities were unobstructed and no new organisms were found. Irregular uplift could be observed in the right nasopharyngeal wall, and the right pharyngeal recess and eustachian tube disappeared. The patient experienced right ocular abduction disorder, with no additional obvious abnormalities.
Laboratory examinations
The quantitative index of Epstein Barr (EB) virus nucleic acid before treatment was higher than the normal value and the quantitative index of EB virus nucleic acid droped to a normal level after treatment. The other laboratory examinations showed no obvious abnormalities.
Imaging examinations
On January 5, 2020, the patient underwent an MRI examination of the nasopharyngeal area. MRI of the nasopharynx and neck showed that the nasopharynx mass was located on the right side, accompanied by skull base bone, and invaded the right intracranial vertebrate. T1WI signal of the sellar dorsum, cavernous sinus, clivus, and right petrous apex decreased, and the tumor entered the right middle cranial fossa through the right cavernous sinus. Multiple enlarged lymph nodes were found in the bilateral parapharyngeal, bilateral neck, and left supraclavicular fossa, and metastasis was considered (Figure 1A).
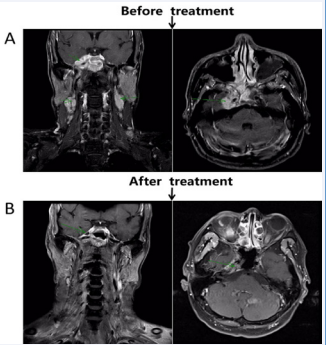
Figure 1: The patient shows a complete response following chemoradiotherapy. A: Extent of lesion invasion before treatment (green arrow); B: The image shows a complete response after treatment.
On January 12, 2020, the patient underwent computed tomography (CT) examination of the chest, abdomen, and pelvis in our hospital. CT showed multiple spots and patches in the posterior segment of the upper lobe tip of the left lung and near the bronchus of the right upper lung. There were multiple nodules and cords in both upper lungs. Because that the secondary pulmonary tuberculosis may be large, the lesions were mainly proliferative foci. No obvious abnormality was found in the abdomen (Figure 2A).
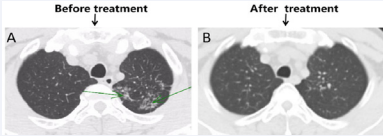
Figure 2: The lesion significantly decreased following anti-tuberculosis treatment. A: Extent of lesion invasion before treatment (green arrow); B: After treatment, the image shows a few old fibrous foci in the middle lobe of the right lung.
Fiberoptic bronchoscopy
Bilateral bronchial mucosa showed inflammatory changes. Acid fast bacilli were not detected in alveolar lavage fluid. No acid-fast bacilli were found in the sputum. Cellular tuberculosis immunoassay showed tuberculosis specific antigen 48 (ESR 24 mm / h).
Final diagnosis
A biopsy of the nasal mass showed non-keratinizing undifferentiated carcinoma. Combined with imaging findings, nasopharyngeal carcinoma was clinically diagnosed as T4N3M0 IVa stage with secondary pulmonary tuberculosis.
Treatment
The patient began to receive three cycles of induction chemotherapy on January 17, 2020. The specific chemotherapy regimen was 350 mg d1 of albumin paclitaxel combined with continuous 120 h pump injection of 5.5 g of 5-FU and 45 mg d2 od lobaplatin (T: Paclitaxel; P: Lobaplatin; F: Pentafluorouracil; TPF scheme).
In February 2020, the patient used 2HRtE / 7HRt (H: isoniazid; Rt: Rifampicin derivative; E: Ethambutol) anti-tuberculosis treatment. On March 18, 2020, the same period of radiotherapy and chemotherapy started, with 68 Gy of radiotherapy and 45 mg of lotplatin for three cycles, combined with targeted therapy of 200 mg nituzumab once a week. During treatment, the patient demonstrated grade II leukopenia, radiation oral mucositis grade 2, and radiation dermatitis grade 1. Five months after the end of the course of treatment, the patient showed a complete response (Figure 1B).
Outcome and follow-up
Positron emission tomography in May 2021 (16 months after diagnosis) showed old tuberculosis in the upper lobe of the left lung and a few old fibrous foci in the middle lobe of the right lung (Figure 2). There was no sign of tumor recurrence or metastasis in the entire body (Figure 3).
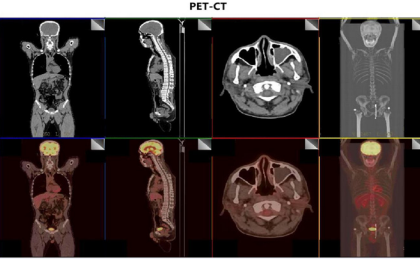
Figure 3: The latest positron emission tomography shows no signs of recurrence or metastasis.
DISCUSSION
The dysfunction or failure of cancer specific T cells in advanced malignant tumors has shown to lead to tumor immune escape and metastasis [2-4]. Tuberculosis is a disease produced by the imbalance of cellular immunity in the body [5]. The immune function in the body plays an important role in the development of diseases. Because immune factors are involved in the occurrence of tuberculosis and advanced malignant tumors, the probability of tuberculosis increases with the occurrence of secondary malignant tumors. Clinically, the related reports of nasopharyngeal carcinoma complicated with secondary pulmonary tuberculosis are rare, and its multimodal treatment has always been a hot topic. Concurrent radiotherapy and chemotherapy are often used for the treatment of advanced nasopharyngeal carcinoma, and the treatment of pulmonary tuberculosis requires multi-drug combination treatment, which should fully consider the patient’s tolerance and prognosis. At present, for tumors complicated with tuberculosis, most adopt simple anti-tuberculosis treatment or tumor treatment, and some adopt intermittent treatment, with general therapeutic effect. Some previous studies have found that the effectiveness of simultaneous treatment was significantly better and that the simultaneous treatment was feasible [6]. In the same period of time, simultaneous treatment can improve the symptoms of pulmonary tuberculosis, improve tolerance, control the progress of pulmonary tumors, and improve the effect [7]. In the present study, patients with nasopharyngeal carcinoma received a TPF scheme for three cycles, which was combined with anti- tuberculosis treatment. The anti-tuberculosis treatment regimen consisted of 2HRtE / 7HRt. Afterwards, the patient received concurrent radiotherapy and chemotherapy, and present with grade II leukopenia during the treatment period, radiation oral mucositis grade 2, and radiation dermatitis grade 1. The anti- tuberculosis drugs isoniazid and rifampicin can produce bone marrow suppression and lead to the decline of blood cells [8,9]. Our results found no serious myelosuppression in the patient, and the course of treatment was tolerable. Through follow-up observation, the tumor completely responded and the pulmonary tuberculosis lesions were stable, without obvious long-term complications.
Through the present case, we believe it is necessary to formulate an appropriate treatment regimen according to the general situation of the patients. In the case of tolerable patients, simultaneous anti-tumor and anti-tuberculosis treatment may be feasible.
AUTHORS’ CONTRIBUTIONS
SHW and LCX contributed equally to the research; SHW collected the patient’s clinical data as the patient’s radiologist; LCX and FZZ reviewed the literature and contributed to manuscript drafting; LH and WYL interpreted the imaging findings and was responsible for the revision of the manuscript; all authors issued final approval for the version to be submitted.
REFERENCES
- Cadelis G, Ehret N. Concomitant discovery of lung cancer and tuberculosis in a cannabis smoker. Rev Pneumol Clin. 2015; 71: 301- 305.
- Ahmadzadeh M, Johnson LA, Heemskerk B, Wunderlich JR, Dudley ME, White DE, et al. Tumor antigen-specific CD8 T cells infiltrating the tumor express high levels of PD-1 and are functio nally impaired. Blood. 2009; 114: 1537-1544.
- Prado-Garcia H, Romero-Garcia S, Aguilar-Cazares D, Meneses-Flores M, Lopez-Gonzalez JS. Tumor-induced CD8+ T-cell dysfunction in lung cancer patients. Clin Dev Immunol. 2012; 741741: 2012.
- Thommen DS, Schreiner J, Philipp Müller, Herzig P, Roller A, Belousov A, et al. Progression of Lung Cancer Is Associated with Increased Dysfunction of T Cells Defined by Coexpressio n of Multiple Inhibitory Receptors. Cancer Immunol Res. 2015; 3: 1344-1355.
- Feng P, Yan R, Dai X, Xie X, Wen H, Yang S. The alteration and clinical significance of Th1/Th2/Th17/Treg cells in patients with multiple myeloma. Inflammation. 2015; 38: 705-709.
- Wu L, Li M, Liu D, Jiang M, Liu Y, Li Z, et al. Treatment of nasopharyngeal carcinoma with pulmonary tuberculosis and gout: A case report. Oncol Lett. 2014; 8: 753-757, 2014.
- Wei Jing, Tao Yuan, Mei Hui, Fu Yingmei, Zhao Jizi, Zhang Wenli, Zhang Fengmin. Research progress on the interaction between tuberculosis and lung cancer. Journal of Practical Oncology. 2018; 32: 340-343.
- Yakar F, Yildiz N, Yakar A, Zeki K?l?çaslan. Isoniazid- and rifampicin- induced thrombocytopenia. Multidiscip Respir Med. 2013; 8: 2013.
- Kuwabara G, Tazoe K, Imoto W, Yamairi K, Shibata W, Oshima K, et al. A Case of Isoniazid-induced Immune Thrombocytopenia. Intern Med. 2021; 2021.









































































































































