Maxillary Sinus Mucocele 4 Cases Reports
- 1. Department of Medicine, Badji Mokhtar University- Sidi Achour, Algeria
ABSTRACT
Maxillary sinus mucocele is a benign, expansile mass which can occur as a result of trauma, spontaneous obstruction of a sinus tract or idiopathic. The purpose of work was describing four cases of maxillary sinus mucocele. We report epidemiologic, clinical, surgical treatment with review of literature.
KEYWORDS
Sinus mucocele; Facial traumatic; Endonasal endoscopic surgery; Caldwell Luc
CITATION
Kharoubi S (2022) Maxillary Sinus Mucocele 4 Cases Reports. Ann Otolaryngol Rhinol 9(4): 1298.
INTRODUCTION
The mucocele is pseudocyctic lesion with a secretive epithelial layer filled with a dense liquid aseptic and slimy mucous. It is an expanding pathology slowly destroying the sinus walls. Frontal sinus is the first location (60%), Ethmoidal sinus (30%) and Maxillary sinus 10% ().The pathogeny of mucocele is related to the association of ostial obstruction and inflammation. Diagnosis is facilitated by computed tomography and surgery is the principal treatment.
PATIENTS AND METHODS
The study population comprises 4 patients (2 males and 2 female, age-range 31-69 years). Mean duration of disease is 10 years (3 to 20 years).
All patients were submitted to diagnostic anamnesis approach, facial examen, nasal endoscopy and computed tomography (CT) (Figure 1).

Figure 1: CT axial plane: right maxillary mucocele (medial wall).
Figure 2

Figure 2: CT coronal plane: right maxillary mucocele (superior part of sinus).
Figure 3
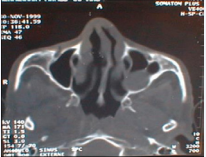
Figure 3: CT axial plane: left maxillary mucocele (posterior part of sinus).
Figure 4
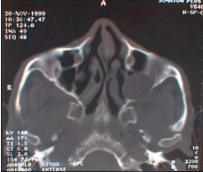
Figure 4: CT axial plane: left maxillary sinus mucocele (lysis of post sinus wall).
In 2 patients the case history was positive for facial trauma, 1 patient with caldwell luc surgery 20 years ago. Clinical presentation found nasal obstruction (2 cases), pain (2 cases), rhinorrhea (1 case), facial swelling (1 case).
RESULTS
All patients submitted to marsupialization of the mucocele by sub labial approach, antrostomie, mucous excision and large meatotomy. Anatomopathologic study confirmed mucocele diagnosis. No recurrence reported after 2 years of Follow up.
DISCUSSION
The maxillary sinus mucocele is related primarily to classic (Caldwell luc), endoscopic surgery and facial traumatic events. Butugan colliged the most important series 16 cases, Busaba and Salman 13 cases [1,2].
The aetiopathologic mechanism associated two factors: ostial dysfunction (tumors, trauma, infection, malformation, dental disturbance, surgical complications) and inflammation. Idiopathic sinus mucocele is reported in the literature after negative investigation (anamnesis and rhinologic exam, CT and RMN). We believe that principal pathogenic factor is mucous liquid that induce hyper pression, hypoxic cellular lesion of sinus mucosa inflammation again and liquid hyper secretion (Diagram 1).
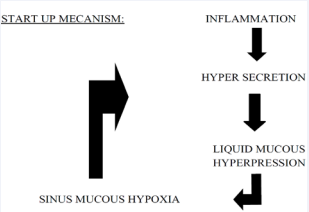
Diagram 1: Mucocele pathogenesis (proposal mecanism).
Patrocinio and AL reported in 2008, the first case of maxillary sinus mucocele in 4-month infant with non-predisposing factors (probably congenital form) [3].In the child maxillary sinus mucocele is uncommon and can to be reported in cystic fibrosis, facial trauma or after endonasal surgery.
Symptomatology is not specific. We can found nasal obstruction, rhinorrhea, epistaxis, facial pain, facial deformation, proptosis, peri orbital swelling, epiphora, palatal deformity, dental problems or radiologic discovery. Nasal endoscopy shows anomalies of lateral nasal way (disformed). Computed tomography in the axial and coronal plane gives a reliable extension balance, the sinus is enlarged with wall blowed reduced or interrupted. Its contents isodense or hypodense and no contrast enhancement, unless infected.
Moreover, MR images showed intermediate signal intensity on T1 and T2, implying the CB is filled with higher protein content of mucocele.MRI is the principal examine for differential diagnosis with neoplastic lesions.
We can report some complications associated to maxillary sinus mucocele: orbital complications (diplopia, proptosis, and visual loss), palatal destruction, dental complications, neuropathic pain (inflammation pterygo-maxillary plexus) [4].
Surinfection of mucocele can induce maxillary sinus mucopyoceles (staphylococcus aureus, alpha hemolitic streptococci, hemophilus spp, and gram negative bacilli or anaerobes- peptostreptococcus spp) [5].
Maxillary sinus mucocele can to be associated with polyposis, osteoma, and malignant tumors [6].
Differential diagnosis is make with cysts (congenital or dental), expansile masses, erosive lesions, benign tumors (polyps, papillomas), sinonasal carcinoma [1,6].
In the past years elective treatment was sub labial approach (Caldwell Luc) with total removal of the sinusal mucous membrane and inferior antrostomy (ventilation, drainage). Actually this technique has been replaced by endoscopic marsupialization (reduced morbidity) [1,2].
CONCLUSION
Mucoceles of the maxillary sinus usually is uncommon and rarely producing symptoms. In such cases, routine radiographs with advanced imaging modalities like computed tomography and magnetic resonance imaging helps in accurately diagnosing the condition. Etiology is unclear and management based in endoscopic endonasal marsupialization. Marsupialization with establishment of ostial drainage relieves the symptoms of the mucocele and also prevents the reaccumulation of mucus. In few cases external approach (sub labial or caldwell luc) is recommended (extensive mucocele, involving facial soft tissues, pterygomaxillary fossa, recurrence).
REFERENCES
- Butugan O, Minoru Takeuti M, Ganz Sanchez T, Rzende de Almeida E, Medicis da Silviera, JA Miniti. A Mucocele du sinus maxillaire. Rev Laryngol Otol Rhinol. 1996 ; 117: 11-13.
- Busaba NY, Salman SD. Maxillary sinus mucoceles: clinical presentation and long-term results of endoscopic surgical treatment. Laryngoscope. 1999; 109: 1446-1449.
- Lucas Gomes Patrocinio, Priscila Garcia Damasceno, José Antonio Patrocinio. Maxillary mucocele in a 4-month infant. Braz J Otorhinolaryngol. 2008; 74: 479.
- López-Valverde A, Gómez de Diego R, Montero J, Albaladejo A. Neuropathic pain associated with mucocele in the maxillary sinus. J Clin Exp Dent. 2010; 2: e142-5.
- Brook I, Frazier EH. The microbiology of mucopyocele.Laryngoscope. 2001; 111: 1771–3.
- RH Khonsari, P Corre, P Charpentier, P Huet. maxillary sinus osteoma associated with a mucocele. Rev Stomatol Chir Maxillofac. 2011; 112: 107-9.









































































































































