Rhinolithiasis: About an Observation
- 1. Department of Otorhinolaryngology and Cervicofacial Surgery, Hassan II University Hospital, Morocco
CITATION
Ouahidi Y, Abdellatif O, Hammoud ZC, El Amine Elalami MN (2022) Rhinolithiasis: About an Observation. Ann Otolaryngol Rhinol 9(1):
1280.
CLINICAL IMAGE
Rhinolithiasis is defined as a solid mineralized calcium concretion, which is formed from progressive deposition of calcareous salts around a central endogenous or exogenous foundation, of variable shape and size [1,2]. It is a rare pathology that often manifests as a unilateral nasal symptomatology of chronic evolution [3]. The diagnosis is based on endonasal examination and the treatment is surgical [4].
We report the case of a 28-year-old female patient, with a history of removal of a neglected right nasal foreign body at the age of 10 years, revealed by an anterior homolateral purulent rhinorrhea, fetid and recurrent after cessation of antibiotic treatment, associated with a chronic homolateral nasal obstruction. The evolution was marked 5 years later by the reappearance of the same symptomatology. Right anterior rhinoscopy revealed a brownish mass of stony consistency with a rough surface surrounded by an inflammatory granuloma occupying the inter septo-turbinal space. The CT scan of the face revealed a well-limited, calcium-dense opacity measuring 1.5 cm in length (Figure 1),
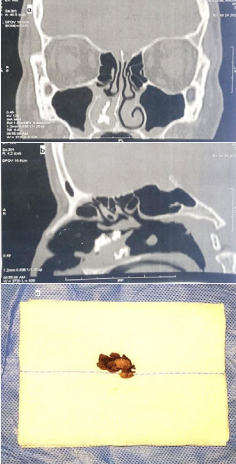
Figure 1: (a) – Nasal CT scan in coronal reconstruction showing rhinolith in the right nasal cavity. (b) - CT scan in sagittal reconstruction of the facial mass showing Rhinolithiasis in the right nasal fossa. (c) - Aspect of the rhinolith after extraction.
retracted over the right middle and lower meatus and associated with a middle ostio-meatal inflammatory remodeling with reactive filling of the right maxillary sinus. This led us to make the diagnosis of rhinolithiasis. The extraction of the rhinolith was performed under general anesthesia, guided by a rigid endoscope (Fig.1). The granulomatous lesions were resected. The patient was put on antibiotics, analgesics, nasal cavity lavage and local corticotherapy to help regeneration of the septal mucosa and to prevent the formation of synechia. The outcome was favorable with 14 months of follow-up.
Removal of foreign bodies would prevent the occurrence of exogenous foreign body rhinolithiasis [4]. Treatment is based on good education of families and children to avoid the introduction of foreign bodies into the nasal cavity. Although rhinolithiasis is a rare condition, it should be considered in the evaluation of patients with long-standing rhinologic symptoms resistant to symptomatic treatment [5].
REFERENCES
1. Kharoubi S. [General review of rhinolithiases]. Ann Otolaryngol Chir Cervicofac. 2008; 18: 34-39.
3. Kaffel N, Khamassi K, Marrakchi J, Selmi Z, Lahiani R, Najeh D, et al. La Rhinolithiase. J Tun ORL. 2010; 25: 59-62.
4. Bakyono KE, Nao E, Zaghre S, Oubian S, Bambara C, Zaghre N, et al. Les rhinolithiases: A propos d’un cas observé au centre hospitalouniversitaire Yalgado Ouédraogo (Burkina Faso). J TUN ORL. 2019; 41: 76-78.









































































































































