Sinonasal Localized Amyloidosis: A Rare Location
- 1. Department of ENT, Hospital Da Senhora Da Oliveira - Guimarães, Portugal
CITATION
Lombo C, Matos C, Fonseca R (2022) Sinonasal Localized Amyloidosis: A Rare Location. Ann Otolaryngol Rhinol 9(1): 1279.
CLINICAL IMAGE
A 71-year-old man presented to the otorhinolaryngology department with a 3-month history of progressive nasal pyramid widening. He denied nasal obstruction, epistaxis and rhinorrhoea. There were no systemic symptoms such as fever, weight loss or night sweats either facial pain or numbness. He had history of ischaemic heart disease and aortic aneurysm. He had non-smoking habits and moderate alcohol intake.
Examination revealed enlargement of nasal pyramid at the level of right nasal bones and cartilageneous vault and anterior rhinoscopy showed a right-sided painless submucosal hard mass occupying the superior meatus and superior aspect of nasal vestibule, as shown in Figure 1.
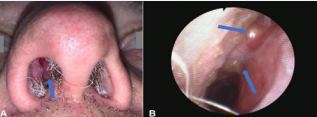
Figure 1: A -Basal view of nasal pyramid demonstrating a right broadening; B - Inferior view of right nasal cavity through nasofibroscopy demonstrating a smooth submucosal mass, occluding superior meatus (arrows).
Remaining ENT examination was otherwise unremarkable. CT-scan findings demonstrated a heterogeneous mass with inside calcifications (Figure 2).
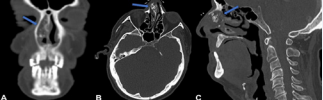
Figure 2: Sagittal (A) and Axial (B) views of paranasal CT scan showing a heterogeneous mass with inside calcifications between nasal septum and nasal bones (arrows).
Incisional biopsy was performed in an outpatient setting and histopathological analysis revealed the presence of amorphous deposits, suggesting the presence of amyloid protein after applegreen birefringence under polarized light in Congo-red stained sections. Patient was then referred for evaluation by Internal Medicine. Systemic amyloidosis was excluded after unremarkable blood counts, biochemistry, erythrocyte sedimentation rate, serum protein electrophoresis and absence of Bence Jones protein in urine analysis. Rectal biopsy specimens, bone marrow aspirates, pulmonary function tests, echocardiography and abdominal ultrasound were also unremarkable. So, the final diagnosis of nasal localized amyloidosis was achieved. Due to cardiovascular disease and absence of symptoms, it was decided to keep the patient under clinical surveillance. After 8 months of follow-up, the lesion remains stable.
Amyloidosis is a group of rare diseases characterized by idiopathic extracellular deposition of insoluble amorphous protein fibrils (amyloid) in multiple organs and tissues. It is usually systemic, but it can be localized to a specific organ or tissue in 10 to 20% of the cases [1]. Localized amyloidosis most commonly occurs at head and neck and it primarily affects larynx and oropharynx. The involvement of nasal cavities is exceedingly rare, with less than forty cases described in literature to date [2]. The pathophysiology of localized amyloidosis is poorly understood, but it has been proposed that light chains are locally produced and deposited by plasma cells. Imaging findings usually consist in well-defined homogeneous soft tissue mass, although it has been rarely reported to appear as heterogeneous and calcified masses, such as the present case. Bony erosion is only reported at advanced stages [3]. Unlike the systemic form, localized amyloidosis generally has good prognosis, rarely progressing to systemic involvement. Evidence regarding localized amyloidosis management is sparse, but it usually involves surgical excision, radiotherapy or clinical surveillance [4].









































































































































