Surgical Management of Failed DCR with Periorbital Abscess and Periapical Abscess - A Complicated Case Report
- 1. Assistant Professor (Eye), Kurmitola General Hospital, Dhaka
- 2. Department of pediatric dentistry, Kumudini Women’s Medical College, Tangail
- 3. Senior consultant (Eye), Cox’s Bazar Medical College, Dhaka
- 4. Interntet Doctor, Saphena Women’s Dental College, Dhaka
ABSTRACT
Purpose: To report the case for guideline for proper diagnosis & management of such a case. A 40 years woman, non-diabetic, non-hypertensive, presented with swelling over the left lacrimal sac region, swelling on the upper left buccal area & watering from the left eye with giving the history of operation (DCR) in the left sac region. Based on the clinical findings, documentation & sac sac patency test, the patient was diagnosed as a case of failed DCR with periorbital abscess & periapical abscess of upper left canine tooth.
KEYWORDS
• Periorbital abscess
• Dacryocystitis
• Osteomyelitis
• Anaesthesia
CITATION
Abul Hasan SM, Mahmudul Hasan SM, Giashuddin M, Afrin S (2017) Surgical Management of Failed DCR with Periorbital Abscess and Periapical Abscess - A Complicated Case Report. Ann Otolaryngol Rhinol 4(1): 1161.
INTRODUCTION
Dacryocystitis mostly occurs in female due to anatomical background & lack of ocular hygiene. Sometimes periapical abscess is complicated to periorbital abscess if treatment is delayed. Continuous infective discharge from the affected eye is cosmetically unpleasant & medico legally problematic. Acute attack with severe pain, osteomyelitis & orbital cellulitis may be complicated if a chronic dacryocystitis is not managed properly. The second time operation is highly technical if first time is not properly done.
Causes of failed DCR are i) inappropriate size and location of bony osteum ii) scarring in the anterior & posterior lacrimal sac wall iii) scarring at the osteotomy site iv) sump syndrome v) common canalicular obstruction.
CASE PRESENTATION
Mrs. Rina of 40 years gentle lady came to our eye department of Kurmitola General Hospital, Dhaka, Bangladesh on 16th June, 2016 & got admitted eye ward with the history of watering from the left eye for last 4 years and history of operation (DCR) on 10th January, 2014 from Nirapod Hospital, Mymensing. The patient also complains of pain with swelling in the buccal region for 3 days. The result of SPT is blocked, swelling over the left sac region, feeling of cystic swelling, fluctuation test is positive, mild tenderness on the periorbital region was present. There was apical abscess on the upper left canine tooth. The patient was counseled about the diseases and their complications, causes of failure of previous operation and further surgical management with importance of follow up [1].
Operation Procedure
Extraction of affected upper left canine tooth was done for periapical abscess under local anaesthesia with coverage of Ing Ceftriaxion-1 gm IV; 12 hourly for 5 days and tab. Etoricoxib-120 mg ;twice daily for relieve of pain with an anti ulcerant [2]. After seven days revision of the failed DCR surgery and periorbital abscess drainage were done at the same setting. This operation started with infiltrating local anesthesia (Figure 1).

Figure 1: Swelling of the buccal region.
The skin incision & muscle retraction was done properly. Huge amount of pus in the periorbital region was drained properly & 5 ml of pus was collected in disposable syringe for C/S & cytology. In our case, the cause of failed DCR was inappropriate size and location of bony osteum & scarring at the osteotomy site. The osteum size was enlarged and margin of the scaring osteum was thoroughly cleaned up. Intubation of silicone tube was done for maintain of patency of the lacrimal drainage system. Then nasal mucosa is anastomosed with remaining sac & muscle. The muscle & skin was opposed properly. The result of culture & sensitivity was no growth of any pathogenic bacteria & cytology reports showed the background sheets of polymorphos & there was no malignant cell. Cefixime, flucloxacillin & metronidazole were used systematically postoperatively & moxifloxacillin eye drop used topically. After 6 weeks the silicone tube was removed. Now the patient is well & SPT is patent after repeated follow up [3].
CONCLUSION
Management of failed DCR with periorbital abscess & periapical abscess were done by a team of eye specialists and dental surgeons. The case was well managed with proper preoperative evaluation & appropriate surgery & postoperative management. A detailed history, through examination & relevant investigation are necessary to confirm the diagnosis & proper management in time is mandatory for the safety of the patient.
DISCUSSION
The extension of orofacial infection to the orbit cans resulting significant morbidity and mortality [4-7]. Periorbital abscess is defined as an abscess in the soft tissue anterior to the orbital septum. It results from the periorbital or periseptal cellulitis which is not treated urgently or by inappropriate antibiotics (Figure 2).
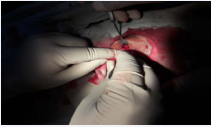
Figure 2: Drainage of periorbital abscess.
(Figure 3).

Figure 3: The procedure of failed DCR
This type of periorbital abbcess may occur from periapical abscess extension via hematogemonus route [8]. In DCR operation, intubation is commonly practiced in chronic dacryocystitis and failed DCR. Linberg and Colleagues2 documented that surgically created ostia (average 11.84 mm diameter) undergo remarkable narrowing during the 1st few months of healing. Mc laschlan3 reported the higher incidence of common canalilcular obstruction as a cause of DCR failure. This obstruction can overcome by intubation. In our cases the causes of failure indentified and treated surgically with intubation [9].
REFERENCES
1. Suresh D. Lacrimal drainage surgery. 2014; 30-36
2. M.J. Roper-Hall. Stallard’s. Eye surgery. 2001; 149-157.
3. Journal of the ophthalmological society of Bangladesh (JOSB). V-39; 64-66.
4. Neelima, Anil Malik. Textbook of Oral and Maxillofacial Surgery. 2012; 663-666.
5. R. Rajendran, Sivapathasundharam B. Shafer’s textbook of oral pathology. 2006; 682-683.
6. Gustav O. kruger. Textbook of oral and maxillofacial surgery. 196-202.
7. Journal of oral maxillofacial surgery.1992; 50:172-178
8. Common Dental Emergencies. Am Fam physician. 2003; 67: 511-517. 9. JOSB; 2014; 41; 219-221.









































































































































