Validation of Identification of Bell
- 1. Department of Family and Community Medicine, University of Toronto
- 2. North York General Hospital, Toronto
ABSTRACT
Previous studies have showed a significant proportion of Bell’s palsy patients are left untreated and suffer from lifelong complications. The study objectives were: 1) to assess the feasibility of finding Bell’s palsy patients in large EMR databases and 2) measure the level of completeness and accuracy of recorded data in Canadian Family Practice EMRs about Bell’s palsy; we used a primary care EMR based database to identify patients with a diagnosis of Bell’s palsy. Nine practices with at least 4 cases of Bell’s palsy per physician participated; 33 patients identified with Bell’s palsy were selected as cases and 220 age and sex matched patients with no of Bell’s palsy diagnosis were selected as controls. We identified 30 true positive Bell’s palsy cases, 3 false positive cases, and 220 true negative cases. Approximately 44.8% of patients were not treated with steroids; they had antivirals alone, had other treatments, or were untreated. Bell’s palsy patients could be reliably identified in EMR derived large health databases
KEYWORDS
EMR, Prednisone, Acyclovir, Bell’s palsy, Fascial palsy
CITATION
Bharathi R, Sullivan F, Aliarzadeh B, Greiver M (2016) Validation of Identification of Bell’s palsy Cases in Canadian Primary Care EMR Data-A Pilot Study. Ann Otolaryngol Rhinol 3(1): 1082.
INTRODUCTION
With increasing use of EMRs in research, not only is accuracy and completeness highly desirable, but to use it as a resource to solve problems facing primary care today is critical [1]. Many studies have used EMRs to explore and investigate various acute and chronic conditions and how they are managed. Once such study explored the management of Bell’s palsy in the UK. During a 12-year period, over 14,000 Bell’s palsy cases were identified and the prescription trends were analyzed. Researchers found that approximately 44% of people diagnosed with Bell’s palsy were untreated (Figure 1) [2].
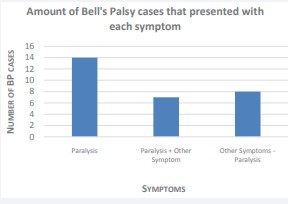
Figure 1: Number of Bell’s palsy cases grouped by presenting symptoms. “Other symptoms” included hearing sensitivity, neck and back pain, and weakness. A total of 21 cases presented with facial paralysis, and 8 cases did not have paralysis but showed other symptoms.
There is mounting evidence that suggests early treatment for the symptoms will cure the paralysis or weakness, however, 20-30% of affected people risk long-term paralysis if untreated [3]. The primary objective of this study was to validate the algorithms used to identify Bell’s palsy patients from electronic medical records (EMRs). We were also interested in the level of completeness and accuracy of recorded data in Canadian Family Practice EMRs about Bell’s palsy. The third objective was to determine if any information on management of Bell’s palsy is recorded in the patient chart; what is the level of completeness of treatment data, and if the condition is treated effectively with steroids, other treatments, or if it is untreated.
BACKGROUND
Bell’s palsy (BP) is a condition that occurs when there is damage to the seventh cranial nerve and results in temporary facial paralysis. The incidence is 20-30 cases per 100,000 per year. It affects both sexes equally but pregnant women and people with diabetes are affected more frequently. The exact cause of this condition is not known, however, it has been suggested by some studies that the herpes simplex virus Type 1 is responsible for inflammation and damage to the facial nerve [4].
In the past few decades, treatments for Bell’s palsy included steroids such as prednisone, anti virals such as acyclovir, other medications or no treatment [5]. While most cases (70%) can be resolved without treatments, a significant number (30%) suffer from partial paralysis or weakness that can be life-long [1]. Recent studies suggest treatment with steroids alone have a significant impact on recovery rate. In a recent clinical trial94.4% of patients treated with prednisone recovered fully after 9 months, compared to 81.6% with no prednisone in the same period. Those treated with and without acyclovir had very little difference, 85.4% and 90.8% respectively [6].
METHODS
We used patient electronic chart review as a gold standard method to measure sensitivity and specificity of identifying Bell’s palsy patients using EMR data search algorithms. The study sample was identified using data from the Canadian Primary Care Sentinel Surveillance Network (CPCSSN) database and additional data collected from providers’ EMR systems. CPCSSN is a Canada-wide primary care research initiative that collects EMR information from participating providers [7]. The goal is to improve the quality of care for patients who are suffering from specific chronic and neurologic conditions. There are 10 regional networks across Canada associated with CPCSSN, and data from the University of Toronto Practice Based Research Network (UTOPIAN) CPCSSN database was used in this study to identify BP cases. UTOPIAN has 14 institutions associated with it [8] and 210 family physicians in 15 health organizations (FHTs/FHOs) are providing data to UTOPIAN-CPCSSN database, including North York Family Health Team (NYFHT), which was the primary site of data collection. Informed consent was obtained from the practices for on-site re-identification of study sample and accessing their medical records for patient chart review.
Study Population
The cases were identified via the CPCSSN database then age and sex matched with 8 control cases each.
Data Abstraction
We first identified cases of Bell’s palsy in UTOPIAN-CPCSSN database by using an algorithm developed and tested by UTOPIAN clinical data specialist [9]. Billing diagnosis, encounter diagnosis, health conditions data and patient problem lists were searched for free-text or coded Bell’s palsy diagnosis. Possible cases were identified using the ICD9 (International Classification of Diseases, 9th version) code 351 or Bell’s palsy as free text. Diagnoses of other causes of unilateral facial nerve paralysis, such as Lyme disease, Ramsay-Hunt syndrome or rarer causes were excluded. Patients age 16 or over were included in this study. This search generated a list of 588 patients with a history of BP. A random sample of participating providers (9) who had more than 4 BP patients in this list was selected from NYFHT; age and sex matched controls with no BP diagnosis as defined by the algorithm were also selected from every practice.
a. UTOPIAN facilitators worked with the research team to identify practices willing to allow access to their EMR and paper records for the purpose of full patient chart review. With the practices’ permissions the Research Assistant (RA) extracted the data. The case record review of both identified cases and controls was undertaken using a standardized abstraction form to 1) determine whether the patient has Bell’s palsy history; and for those with a Bell’s palsy history 2) describe the following Signs and symptoms (date and severity)
b. Diagnosis (date and details)
c. Treatments (before and after diagnosis, medication name, dosage, frequency, duration, referrals, and number of medical visits)
Further details were extracted through letters from encounters at the ER and from specialists such as ENT and neurology. The criteria for false positive cases was if the cases were identified in the CPCSSN database as positive for BP but through the case-note review the information suggested (providers’ and specialists’ notes) that it was not BP, and then it would be recorded as false positive.
The two EMR systems used were Nightingale on Demand (NOD) and Practice Solutions Suit (PSS). The RA had a list of identified cases that were coded with ICD-9 code 351 and their controls. First, the RA would identify the case chart and look for the diagnosis code and the date of diagnosis. Then, diagnostic and treatment details were extracted to check whether the diagnosis was appropriate. Information from referral reports from specialists, such as neurologists, were used to identify false positives. Data for control patients were extracted in the same manner. However, instead of confirming the diagnosis code through encounter details, the RA searched for any encounter related to facial paralysis/weakness. EMR charts for all case and control patients with data from 2006 to 2015 were reviewed.
Abstracting treatment information consisted of reviewing the treatment section of the case chart in the EMR. Cases that were prescribed steroids, anti virals, eye patch, other treatments, combinations, or no treatment were noted in separate columns. The parameters of whether a case was effectively “treated” or “untreated” were: if the Bell’s palsy case was prescribed steroids, anti virals, or a combination of both after diagnosis of BP, it was a treated case; if the Bell’s palsy case had other treatment such as massages, eye patch, other treatments or none, it was untreated. These parameters were chosen so comparison to the UK study would be possible. Data were analyzed to demonstrate the trend of prescribed treatments over time for Bell’s palsy in Canada and compare it to results from the UK.
RESULTS
Data were abstracted from a total of 253 patients in 9 different primary care practices patient charts; 33 of these patients were Bell’s palsy cases identified in UTOPIAN-CPCSSN database by search algorithms, and the rest were 220 age, sex matched controls. Of the 253 cases 72% (182) were female and 28% (71) were male (Table 1).
Table 1: Number of BP cases and controls grouped by sex with BP and the control cases.
| Control | BP Cases | |
| Male | 60 | 11 |
| Female | 160 | 22 |
Of 33 identified BP cases, 3 were false positives. Of 30 true BP cases, 63.3% (19) were female and 36.6% (11) were male, 43.8% (13) were aged 60 or older and 56.2% (17) were between the ages of 24 and 60, and 72.4% (21) showed symptoms of unilateral paralysis only or with other symptoms, and 27.6% (8) did not present with unilateral paralysis but had other symptoms (Figure 1). 29 out of 30 Bell’s palsy cases had prescribed medication records for various conditions. Of that 29, 62.1% (18) were treated for their BP diagnosis with steroids, anti virals or a combination of both, and 37.9% (11) had no treatment information recorded or had received other treatments (Figure 2).
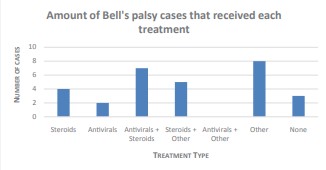
Figure 2: Number of BP patients grouped by treatment type. 18 cases were prescribed steroids and/or antivirals, while 11 cases were prescribed other treatment or were untreated.
There was no false negative control and only 3 false positive BP cases, the sensitivity of developed algorithm was 100%, and the specificity was 98.65% (Table 2).
Table 2: Validation of BP case-finding algorithm
| Statistics | Value | Value |
| Sensitivity | 100` | 88.4 – 100 |
| Specificity | 98.6 | 96.1 – 99.7 |
| PPV | 90 | 75.7 – 98.1 |
| NPV | 100 | 98.3 – 100 |
The time between the onset of symptoms and presentation was recorded in 28 cases, ranging from the same day to 12 days with a mean time to presentation of 3.1 days. Most cases of Bell’s palsy presented to the emergency room, and the next most common place of presentation was a walk-in center or family physician’s office. The diagnosis was usually made at the time of presentation and referral for a specialist opinion was made if uncertainty remained.
DISCUSSION
We found using search algorithms in large health databases derived from two primary care EMRs in Canada is a feasible method with high sensitivity (100%) and specificity (98.6%), with CI = 0.95, to identify BP patients. The completeness and accuracy of the information was explored through individual chart reviews. We found that treatment information was recorded for a large number of BP patients by their family doctors in EMRs, and additional information about the management of the condition, i.e. specialist referrals, were also recorded. The final objective was accomplished by analyzing the prescription patterns for each positive case. The percentage of untreated BP cases in our sample is 38% that is somewhat similar to what a previous study found in UK. In that study 44% of BP patients were left untreated [2]. According to our data, over half (57.1%) of those who received treatment were prescribed steroids (Prednisone) alone or with a combination of anti virals (Valtrex), this compared favorably with reported treatment in the UK which mainly consisted of Prednisone and/or Acyclovir. Cases that were not treated with steroids (44.8%) received other forms of treatments such as, anti virals alone, eye patches, massages, physical therapy, acupuncture, or none at all. While there was an effective treatment method on the market, still 45% of people diagnosed with Bell’s palsy were not treated with steroids.
There are a number of limitations for this study. One main limitation of this study was the small sample size. Management information for some cases, both BP and control, were not available due to reasons such as: patients had moved and are under a different provider, or could not be located in the EMR system. It is possible that some patients received treatment from other care providers (i.e. hospital emergency unit or walk-in clinics) that is not recorded in patient chart. Better representation of Bell’s palsy incidence in Canada and management information can be obtained if larger samples from different regions of Canada, with data linkage to hospital data could be used.
We understand that some reasons for this lack of steroid use can be patient preferences and the fact that BP presents as an acute condition and can be resolved on its own. But long-term complications are common, and could be reduced by proper treatment [10]. Overall, primary care EMRs had complete and accurate patient information and detailed notes of encounters with various specialists. This allowed us to discover that 38% of the patients diagnosed with Bell’s palsy were not treated effectively with steroids or anti virals. Further research is required to investigate more in-depth into prescription patterns and the development of a scheme to help primary care providers treat these cases and other acute conditions. Additionally, we plan on conducting a multi-national comparison of prescription patterns for BP in the UK, Canada, and the Netherlands to further explore and develop schemes and interventions for different populations that cannot only improve the management of this condition, but other similar acute conditions as well.
ACKNOWLEDGEMENTS
Thank you to Ivanka Pribramska for providing admin support and Christopher Meaney for statistical analysis. Funding for this study was provided by North York General Hospital Research Exploration Fund.









































































































































