Crescentic IgA Nephropathy Flare up with ANCA Positivity after Covid-19 Infection
- 1. Associate in Kidney Care, Des Moines, Iowa, USA
CITATION
Arjun Sekar (2021) Crescentic IgA Nephropathy Flare up with ANCA Positivity after Covid-19 Infection. Ann Clin Pathol 8(1): 1155.
INTRODUCTION
A 32-year-old lady presented with 4 weeks of cough and generalized weakness. 4 weeks prior, she was diagnosed with a breakthrough covid-19 infection with fever & cough as the main symptoms (2 doses of Pfizer vaccine completed 6 months earlier, which she tolerated well). She had not yet received the booster dose of the vaccine. She received outpatient supportive treatment (no monoclonal antibodies were given) and fevers subsided within 3 days of onset. However, dry cough and weakness persisted, prompting further workup.
CASE REPORT
Labs revealed; creatinine 3.44 mg/dl, CO2-15 mmol/L, acceptable electrolytes, hemoglobin 8.3 g/dl and microscopic hematuria. She had a prior history of IgA Nephropathy (IgAN) which was diagnosed during adolescence and was managed conservatively. She was not on an ace inhibitor or angiotensin receptor blocker as she ran out of medications for 6 months and had not established care with a new physician yet.
A year ago, creatinine was 1.5-1.6 mg/dl. Despite hydration, creatinine few days later increased to 4.15 mg/dl and serologies showed Myeloperoxidase (MPO) Anti-Neutrophil Cytoplasmic Antibody (ANCA) positivity and negative anti-Glomerular Basement Membrane (GBM) titers. C3 (normal 90-180 mg/dl) and C4 (normal is 10-20 mg/dl) was low at 47 and 6 respectively. Vitals were stable and physical examination, unrevealing.
Pulse dose methylprednisolone 500 mg intravenously was begun and kidney biopsy was done 2 days after admission. It showed IgA nephropathy based on Oxford classification score; M1 E0 S1 T1 C1. 14/29 glomeruli showed sclerosis and there was mild to moderate interstitial fibrosis and tubular atrophy. There was one cellular crescent with fibrinoid necrosis (Figure 1) which confirmed the diagnosis of rapidly proliferative glomerulonephritis (RPGN).
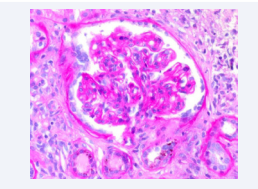
Figure 1: Confirmed the diagnosis of rapidly proliferative glomerulonephritis (RPGN).
Light microscopy diffusely showed mesangial matrix expansion and segmental mesangial hypercellularity (Figure 2). Immunofluorescence showed IgA deposition present in sclerotic and intact glomeruli. These pathological features are consistent with the diagnosis of IgAN.
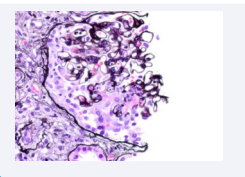
Figure 2: Immunofluorescence showed IgA deposition present in sclerotic and intact glomeruli.
Creatinine was 3.9 mg/dl one week later. She received 3 days of pulse steroids and was transitioned to oral prednisone and cyclophosphamide at 1mg/kg. Symptomatically, she did better and she did not require any dialysis.
DISCUSSION
Most likely, covid-19 infection is what triggered IgA nephritis flare in our patient. Underlying infections can cause flare up of IGAN.
Despite widespread vaccination against covid-19, global infection rates for coronavirus cases remains very high.
De-novo cases of rapidly proliferating glomerulonephritis (RPGN) [1] and flare ups of underlying glomerulonephritis [2] have been reported after coronavirus infections and vaccinations.
Collapsing glomerulopathy is the most common glomerular disease associated with covid19 infection [3]. IgAN flare up post covid19 infection has been reported4 .The exact mechanism of IgAN flare up after covid19 infection is unknown. The increase in inflammatory markers due to a mucosal infection like SARS-Cov2 could lead to abnormal glycosylation of IgA1 antibodies, forming immune complexes with IgG autoantibodies and depositing in the tissues [5].
IgAN with ANCA positivity is generally associated with a worse clinical course [6]. To our knowledge, this is the first case of crescentic IGAN with serum ANCA positivity after coronavirus infection. Research is needed to identify those at high risk of glomerulonephritis flare ups. Timely screening with biomarkers post infection in high-risk individuals could lead to prompt treatment and improved outcomes.









































































































































{kind=link}