A Rare Case of Elective Hernia Surgery: Littre Hernia
- 1. Department of Surgery, Izmir Katip Celebi University, Turkey
Abstract
Meckel diverticulum (MD) is the most frequently seen congenital anomaly of the gastrointestinal system. Littre hernia (LH) is defined as the presence of MD in a hernia sac. Although LH is commonly seen in emergency surgeries such as incarceration and obstruction or hemorrhage, it is rare in elective surgeries. Herein, we present a rare case of MD which was detected during elective inguinal hernia surgery.
Keywords
Meckel diverticulum, Littre hernia, Elective surgery, Inguinal hernia
Citation
Kamer E, Orse A, Er A, Cengiz F, Ozogul M, et al. (2017) A Rare Case of Elective Hernia Surgery: Littre Hernia. Ann Emerg Surg 2(1): 1004.
ABBREVIATIONS
MD: Meckel Diverticulum; LH: Littre Hernia
INTRODUCTION
Meckel diverticulum (MD) is the most commonly seen congenital anomaly of the gastrointestinal system, accounting for 1 to 3% of cases [1]. It occurs due to theimproper closure of the omphalomesenteric duct [1]. It was first described by Wilhelm FabriciusHildanus in 1598 [2]. Incarceration of MD was first described anecdotally in 1700 by Littre, a French surgeon [1,2]. However, this anomaly was named and its pathophysiology was first explained in 1809 by Johann Friedrich Meckel [1]. It frequently occurs on the terminal ileum [2]. It has clinical relevance, as it may cause complications such as intestinal obstruction, diverticulitis, hemorrhage, and perforation [1,2].
Littre hernia (LH) is defined as the presence of MD in a hernia sac [1]. It was first described in 1700 by Alexis Littre; however, the term LD was used for the first time in 1841 by Reinke [2]. About 50% of LH can occur in the inguinal region, 20% in the femoral site, 20% in the umblical site, and the remaining 10% in other locations [3]. In this report, we present a rare case of MD which was detected during elective inguinal hernia surgery.
CASE PRESENTATION
A 62-year-old male patient was admitted to our outpatient clinic with complaints of pain and swelling in his left inguinal region and left inguinal hernia was detected. He had hypertension with no incarceration. His physical examination findings and laboratory test results were normal. A written informed consent was obtained from the patient. He underwent standard preoperative examinations, and elective hernia surgery was performed with left inguinal incision. During surgery, indirect inguinal hernia was detected. Upon opening the hernia sac, omentum and loops of small intestine were found within. A MD of 6-cm in length and 2-cm in size was detected on the wall of the small intestine (Figure 1).
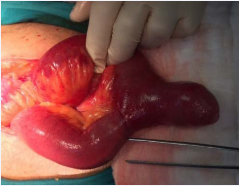
Figure 1: A large amount of small bowel with Meckel’s diverticulum in hernia sac.
Stapler-assisted wedge resection was, then, performed, and followed by inguinal hernia repair using a standard prolene mesh. Stapler was applied to the base of the diverticulum, perpendicular to the base of the diverticulum but transverse to the longitudinal axis of the bowel. The stapler was fired and the diverticulum was resected off the ileum. Small bleeding points at the edge of the staple line, if present, were sutured intracorporeally with 3-0 Vicryl. The postoperative period was uneventful, and the patient was discharged next day. Patient was followed up for 9 months, and was found to be symptom-free.
DISCUSSION
Meckel diverticulum, which is the most frequently seen congenital anomaly of the gastrointestinal system, is a true diverticulum that contains all layers of the intestinal wall [4]. It occurs due to the failure of the omphalomesenteric duct to close, which should take place around seventh to eight weeks of pregnancy [6]. It is usually asymptomatic [4]. The definite diagnosis is made during surgery for complications such as hemorrhage, ulceration, infection or ileus [4]. In adults, 4 to 10% of MD cases are incidentally diagnosed during surgery for other reasons [3]. It is seen twice as much in males as females [4]. Obstruction of the small intestine in adults and hemorrhage in children are most common complications [5,6]. One of the complications of MD is LH, which is observed in 10% of the cases, and is usually seen during infancy [2,5,6]. It most commonly involves the abdomen in infants, and the inguinal region in adults [3,6]. It usually occurs in the right inguinal region [7]. In our case, LH was also localized in the right inguinal region.
In case of incomplete reduction of incarcerated hernias, fecal fistula in hernia, rectal hemorrhage or recurring stomach pain, diagnosis should be made intraoperatively, although LH is initially suspected [3,6]. In the literature, there are reported cases with hemorrhage, obstruction and perforation, and most frequently, incarceration [7-9]; however, the number of cases of LH diagnosis during elective surgery is very limited [9]. In our case, LH was detected during elective hernia surgery.
Treatment is controversial in MD. In patients with symptoms and complications, surgical treatment is indispensible. In case of an incidental diagnosis, there is a consensus on performing resection among pediatric surgeons; however, indication of prophylactic MD resection still remains controversial in adults [3,4]. In case of a broad-based diverticulum, segmental resection is recommended, whereas diverticulectomy would be sufficient in the narrow-based ones. Biel et al. performed wide-V wedge resection in a case with MD which was detected during elective inguinal hernia surgery [9,10]. Similarly, our case underwent wedge resection.
In conclusion, this report highlights that the detection of MD in the hernia sac during elective inguinal hernia surgery is rare and resection of MD is recommended.








































































































































