Concepts that Prevent Inguinal Hernia Formation
- 1. Department of surgery, Poona Hospital & Research Centre, Pune
- 2. Hernia Centre, Poona Hospital & Research Centre, Pune
Abstract
The author was not satisfied with the present concept about the strength of the transversalis fascia that is said to prevent inguinal hernia formation in the normal individuals. Therefore, this study was conducted to see the anatomical status of transversalis fascia and presence or absence of aponeurotic extensions in the posterior wall of the inguinal canals as were described by some stalwarts like Condon, Nehus etc.
Methods: This is a prospective study of 30 inguinal canals opened for inguinal hernia surgery and 30 for varicocoele or lipoma of the cord (No hernia) surgery from January 2007 to December 2012. Inguinal canals were opened under local anesthesia and without any sedation. Lipoma were excised, varicocoele ligated and the hernia repaired by authors technique [1]. Observations were made about the structure of the inguinal canal, more particularly the posterior wall.
Results: 30 inguinal canals opened for lipoma or varicocele surgery without hernia showed full cover of the aponeurotic extensions of varying density and out of 30 inguinal canals opened for hernia surgery, 24 did not show presence of the aponeurotic extensions and 6 canals showed deficient or scanty aponeurotic extensions. None of them had full cover of the aponeurotic extensions. Thin and tiny Aponeurotic fibers seen in the posterior wall of the patient were treated as absent Aponeurotic extensions
. Conclusions: Transversalis fascia does not have any role in the prevention of inguinal hernia formation. Aponeurotic extension in the posterior wall is the principle factor that prevents the inguinal hernia formation.
Keywords
Inguinal canal anatomy; Physiology; Theories that prevent hernia formation
Citation
Desarda MP (2017) Concepts that Prevent Inguinal Hernia Formation – Revisited New Concepts of Inguinal Hernia Prevention. Ann Emerg Surg 2(1): 1007.
INTRODUCTION
Etio-pathology of any disease has importance because that can lead us to find a solution. Therefore, it is important to observe the structural changes (etio-pathology) that has taken place during the process of inguinal hernia formation. The author has already published one article in 2003 on the surgical physiology of the inguinal hernia repair [2]. Researchers postulated various factors to be the cause of hernia formation. In this context, some questions related to those factors still exist. A) Upward and lateral movement of the internal ring and approximation of the crura results in a shutter mechanism at the internal ring [3]. When the arcuate fibers of the internal oblique and transversus abdomen is muscle contract, they straighten out and move closer to the inguinal ligament (shutter mechanism at the inguinal canal) [4,5]. This opposite movement (upward & downward) of the same muscle needs proper explanation. B) The term “obliquity of the inguinal canal” is also not true because the spermatic cord is lying on the transversalis fascia alone throughout its course. C) Repeated acts of crying in children do not result in hernia formation in spite of the almost absent “obliquity of the inguinal canal” or “shutter mechanism”. D) Every individual with a high arch or a patent process us vaginal is do not develop hernia [6]. E) Strength of the transversalis fascia cannot be a real factor when it is papery thin without any strength. F) Factors that are said to prevent herniation are not restored in the traditional techniques of inguinal hernia repair and yet 70–98% of patients are cured. Then what factors play a real role in the prevention of hernia formation? The author studied literature on inguinal canal anatomy extensively and found that the posterior wall of the inguinal canal has another cover of aponeurotic extensions in front of the transversalis fascia. This is not mentioned in various research articles or the text books in surgery. Therefore, the author conducted this study to observe the presence of the normal cover of aponeurotic extensions in posterior wall of the patients with hernia and without hernia.
MATERIALS AND METHODS
Inguinal canals opened under local anesthesia without any sedation were included in this study. Obese, malnourished or patients having recurrent or strangulated hernia were excluded. 30 inguinal canals were opened up for lipoma of the cord or varicocele surgery from January 2007 to December 2012. Patients were between 18-60 years of age with median age of 48.5 years. There were many inguinal canals opened for inguinal hernia surgery during this period but only 30 cases were selected for this study that matched with the age and body type of the no hernia patients (Table 1).
Table 1: Number of inguinal canals studied.
|
Aponeurotic extensions Number of patients Number of patients without inguinal hernia with inguinal hernia Full cover 30 0 Absent 0 24 Partial or defective cover 0 6 |
Five unilateral lipoma of the cord were treated by excision, 15 unilateral and 5 bilateral varicocele by vein ligation and 30 unilateral hernias were repaired by suturing an undetached strip of the external oblique aponeurosis between the internal oblique muscle and the inguinal ligament as described in the author’s technique of the hernia repair [1]. Observations were made and recorded about the structures of the posterior wall. The posterior wall surface was scraped with tooth forceps or gauze piece or scoop after mobilization of the spermatic cord to find out the presence of the aponeurotic extensions in it. Naked eye observations were sufficient to detect the layer of the Aponeurotic extensions and to conclude whether they are present or absent or scanty and deficient. Thin and tiny attenuated aponeurotic fibers if seen in the posterior wall of the patient were treated as absent aponeurotic extensions. If present then it was further explored to find out whether they are giving full cover or a partial cover (Figure 1-3).

Figure 1: Full cover of Aponeurotic extensions seen in normal individuals without hernia.

Figure 2: Scanty aponeurotic extensions resulting in the hernia formation.

Figure 3: Deficient aponeurotic extensions resulting in the hernia formation.
The observations were analyzed to draw the conclusions.
RESULTS
30 canals opened for lipoma or varicocele surgery had all shown full cover of the aponeurotic extensions (Figure 1), though the density of fibers differed in every patient. Transversalis fascia was not seen in those cases as it was behind these extensions. 30 canals opened for hernia surgery had either shown posterior lamina covering the pre-peritoneal pad of fat or the pseudo fascia or the partial or scanty cover of the aponeurotic extensions. Transversalis fascia was not distinctly found in any of the patient after mobilization of the spermatic cord. None of these patients had shown presence of the full cover of the aponeurotic extensions. 24 inguinal canals out of 30 studied did not show the presence of the aponeurotic extensions and 6 canals showed deficient and scanty aponeurotic extensions (Figure 2,3), (Table 2).
Table 2: Distribution of Aponeurotic extensions.
|
Number of patients without inguinal hernia Number of patients with inguinal hernia 30 30 Operated for lipoma of cord & varicocoele Operated for inguinal hernia |
DISCUSSION
The posterior wall of the inguinal canal lying between the inguinal ligament and the muscle arch behind the spermatic cord is mainly formed by the transversalis fascia as a single layer structure, medially enforced by the falx inguinalis. And the strength of this transversalis fascia gives the protection against the hernia formation in the normal individuals. This is the general perception carried by many researchers in their articles. But it is not so in reality. Posterior wall of the inguinal canal is composed of two layers. Transversalis fascia is a posterior layer and in front of it is yet another layer of the aponeurotic extensions from the Transversus Abdominis Aponeurotic Arch (Linear diagram 1),inset.
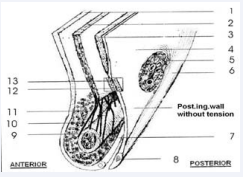
Linear diagram 1: -Section of inguinal canal at rest. SOURCE: Desarda MP. Surgical physiology of inguinal hernia repair – a study of 200 cases. BMC Surg. 2003; 3: 2
External oblique aponeurosis, 2) Internal oblique muscle, 3) Transversus abdominis muscle, 4) Endo abdominal fascia, 5) Internal inguinal ring, 6) Iliopubic tract, 7) Inguinal ligament, 8) Pubic symphisis, 9) Spermatic cord, 10) Interparietal connective tissue (cremasteric fascia), 11) cremasteric muscle, 12) Aponeurotic layer of posterior inguinal wall, 13) Fascial layer of posterior inguinal wall
It is also called as the “Discontinuous part of the Transversus Abdominis Aponeurotic Arch”. The extensions from the conjoint tendon (Falx inguinalis) medially are also a part of these extensions. [7] Deep interest was taken by many stalwarts in the anatomy of the inguinal canal in the first half of the 20th century. Nehus, Condon, MacVay, Anson and many others gave beautiful descriptions about the posterior wall of the inguinal canal. They have all equivocally stated that the transversalis fascia is just an extension of the endo abdominal fascia and is papery thin without any strength. They also have stated about the presence of the Aponeurotic extensions in front of the transversalis fascia in the posterior wall of inguinal canal in the normal individuals. [8,9]
The aponeurotic extensions start from the transversus abdominis and get first inserted on to the inguinal ligament and iliopubic tract and then further extend for second insertion on to the pectineal bone and ligament. Thus it covers and protects the entire myopectineal orifice described by Fruchaud giving protection from inguinal as well as femoral hernias. Absence, presence or attenuation of these extensions is genetically determined and therefore hernias are commonly seen in families. Fruchaud postulated that the myopectineal orifice is inherently weak in such patients, and is genetically determined [10].
Inguinal structures, as living entities that move and function cannot really be appreciated either by dissection on cadavers or operations on patients under general or spinal anesthesia [11]. The precise demonstrations of live movements of the posterior wall and the musculo-aponeurotic structures around the inguinal canal during the acts of internal abdominal ‘blows’ (raised intraabdominal pressure) is so far not possible. The first recorded observation of dynamic activity in the internal ring of a living non anaesthetized human being was done in one patient by Tobin et al., [12]. Many such studies of dynamic activity in the internal ring have been done in dogs [13]. Peacock EE stated that little is known about the muscular activity in the internal ring because the conventional repair of groin hernia does not adequately expose the normal muscle fibers [14]. Preperitonial exposure is, of course, performed in an anaesthetized patient; consequently little information has been acquired about the function of a sphincter muscle, even though the internal ring can be visualized. But it is clearly seen in laparoscopic repair that there are two layers in this floor: a weak transversalis fascial layer and a stronger aponeurotic layer, formed by the variable aponeurotic fibers sent by the arching transvers abdominis muscle. The contribution of the latter determines the strength of the posterior wall of the inguinal canal.
The author found that in 30 canals having lipoma of the cord or varicocele without any hernia had shown full cover of the aponeurotic extensions, though the density of fibers was different in each case and the posterior wall was strong and dynamic. On the other hand, 30 canals opened for inguinal hernias had no full cover of the aponeurotic extensions. They had either absent or deficient aponeurotic extensions and the posterior wall was weak and flabby and adynamic. Naturally, the posterior wall of the canal was not strong enough to give physical protection against the herniation process. The condensed part of the transversalis fascia and the aponeurotic extensions give mechanical strength to the posterior inguinal wall to resist internal abdominal blows [2,8,15]. If aponeurotic extensions are absent, then the transversalis fascia alone cannot resist the internal blows for a long period and herniation occurs.
Secondly, the posterior inguinal wall and the accompanying aponeurotic extensions are physiologically dynamic. Muscular contraction of the transversus abdominis pulls this posterior wall and the aponeurotic extensions upward and laterally creating tension (increased tone) in it (Linear diagram i,ii,iii).
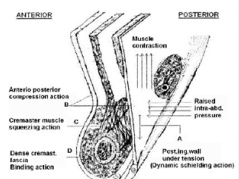
Linear diagram 2: Changes during raised intra-abdominal pressure (Canal in action). SOURCE: Desarda MP. Surgical physiology of inguinal hernia repair – a study of 200 cases. BMC Surg. 2003; 3: 2.
Contraction of transversus abdominis muscle pulls the posterior inguinal wall above and laterally creating tension in it (Dynamic shielding action), B) External oblique aponeurosis and posterior inguinal wall come closer (anterior-posterior compression action), C) Squeezing action and pulling effect of cremasteric muscle, D) Dense and strong cremasteric fascia exerts binding effect on structures in the inguinal canal for their optimal dynamic movements.

Linear diagram 3: Cross section of a strong posterior wall of the canal in normal individuals. (From book “Hernia” with some modifications).
The wall with increased tone in it resists internal abdominal blows better than a wall without such increased tone. This increased tone in the posterior wall is created in gradation as per the force of contraction of the muscles. And the force of contraction of the muscle changes as per the force of the internal abdominal blow. This is important physiological phenomenon. The posterior wall should be described as an independent entity, playing an important role in the prevention of hernia formation, not only because of its physical strength but also because of its dynamic nature. Therefore, any new approach to inguinal hernia repair must consider replacing this absent or deficient aponeurotic element with any other suitable natural structure. Such a physiologically dynamic and strong posterior wall is constructed in the author’s technique of inguinal hernia repair [1].
Robert Bendavid stated that the posterior wall is a tri-layer structure composed of fascial extensions from the internal oblique, transversus abdominis and endo-abdominal fascia i.e. transversalis fascia [16]. The author feels that the fascial extensions from internal oblique cannot be included as part of the posterior wall layer as it will come into the contents of the inguinal canal and not its wall. The cremasteric muscle itself is an offshoot of the internal oblique muscle along with its fascia, the cremasteric fascia. This fascia fills up the spaces between the inguinal canal wall and the spermatic cord. Therefore, the posterior wall is a bi-layer structure, composed of the extensions from the transversus abdominis i.e. aponeurotic extensions and the endo-abdominal fascia i.e. transversalis fascia.
One mistake is often made by the operating surgeons in inguinal hernia surgery. The membrane like condensation of fibrous stroma of preperitoneal fatty or fascial layer (Posterior Lamina) is mistakenly interpreted by some as the transversalis fascial layer [17]. The author is doubtful of finding intact transversalis fascia in the inguinal canals opened for inguinal hernia surgery by the surgeon if these aponeurotic extensions are absent. It gets avulged easily while surgeon mobilizes the spermatic cord and what he sees in reality is the posterior lamina or pseudo fascia.
The author agrees with Robert Bendavid [16] that later investigators and surgeons overlooked this critical observation and the misconceptions of posterior wall as only transversalis fascia, a single layer structure, have been perpetuated in many publications. The misconception is about to treat transversalis fascia alone as the posterior wall of the inguinal canal and giving importance to it as the principle factor that gives protection from the inguinal hernia formation.
There were many researchers who put forward their own theory that was said to prevent the inguinal hernia formation in the normal individuals. Murray [6] blamed high muscle arch as one such factor. Russell [18] blamed patent processus vaginalis or oblique pelvis. Read [19] talked of metastasis emphysema, Cloquet’s [20] lipoma theory and similarly, Peacock’s [21] theory of defective collagen synthesis. But all these theories were not accepted for the want of the adequate and conclusive evidence.
Adynamic and weak posterior wall of the inguinal canal due to absent or deficient aponeurotic extensions from the transversus abdominis aponeurotic arch is the main cause of hernia formation. Reduced strength of the muscles and binding action of the connective tissue are also important secondary factors [2].
CONCLUSION
The posterior wall of the inguinal canal is a bilayer structure composed of the transversalis fascia and the aponeurotic extensions. The aponeurotic extension in the posterior wall of the inguinal canal is the real factor that gives strong and dynamic protection from the herniation. The present study endorses that person having no full cover of the aponeurotic extensions in its posterior wall are prone to develop inguinal hernia.
REFERENCES
- Desarda MP. No-mesh inguinal hernia repair with continuous absorbable sutures: A dream or reality? (A study of 229 patients). Saudi J Gastroenterol. 2008; 14: 122-127.
- Desarda MP. Surgical physiology of inguinal hernia repair – a study of 200 cases. BMC Surgery. 2003; 3: 2.
- Lytle WJ. The internal inguinal ring. Br J Surg. 1945; 32: 441-446.
- Hammond TE. The etiology of indirect inguinal hernia. Lancet. 1923; 204: 1206-1208.
- Keith A. On the origin and nature of hernia. Br J Surg. 1924; 11: 455-475.
- Murray RW. The saccular theory of hernia. Br Med J. 1907; 2: 1385.
- Condon RE. The anatomy of the inguinal region and its relationship to groin hernia. In: Nehus LM, Condon RE (Eds) Hernia. 3rd edn. Philadelphia, PA: JB Lippincott 1989; 14-78.
- Anson BJ, Morgan EH, McVay CB. Surgical anatomy of the inguinal region based upon a study of 500 body-halves. Surg Gynaecol Obstet. 1960; 111: 707-725.
- MacVay CB. Inguinal hernioplasty. Surg Cl N Am. 1966; 46: 1089-1100.
- Fruchaud H. Anatomie chirugicale des hernies de l'aine. Paris, France: Doin Editeurs; 1956.
- Griffith CA. Inguinal hernia: an anatomic-surgical correlation. Surg Cl North Am. 1959; 39: 531-556.
- Tobin GR, Clark DS, Peacock EE Jr. A neuromuscular basis for development of indirect inguinal hernia. Arch Surg. 1976; 111: 464-466.
- MacGregor WW. The demonstration of a true internal inguinal sphincter and its etiologic role in hernia. Surg Gynaecol Obstet. 1929; 49: 510-515.
- Peacock EE Jr, Madden JW. Studies on the biology and treatment of recurrent inguinal hernia. II. Morphological changes. Ann Surg. 1974; 179: 567-571.
- Anson BJ, McVay CB. Surgical anatomy. 5th edn. WB Saunders Co, Philadelphia. 1971; 1: 461-532.
- Robert Bendavid. Transversalis fascia rediscovered. Surg Cl N Am. 2000; 80: 25-33
- Condon RE. The anatomy of the inguinal region and its relationship to groin hernia. In: Nehus LM, Condon RE Hernia. 2nd edn. Philadelphia, PA: JB Lippincott. 1978; 62.
- Russel RH. The saccular theory of hernia and the radical operation. Lancet. 1906; 3: 1197-1203.
- Read RC. Attenuation of the rectus sheath in inguinal herniation. Am J surg. 1970; 120: 610-614.
- Cloquet J. Recherches sur les causes et l’anatomie des hernies abdominales. Paris: Mequignon-Marvis. 1819.








































































































































