Necrotic Epiploica Appendix as the Sole Content of Strangulated Inguinal Hernia
- 1. Department of Surgery, Civil Service Hospital of Nepal, Nepal
- 2. Department of Surgery, Global Hospital, Nepal
Abstract
Background: Small bowel loops or a part of omentum is the usual content of inguinal hernia. However, certain parts of the colon, urinary bladder, vermiform appendix, Meckel’s diverticulum, uterine tube and ovary, and other tissues may be observed in a strangulated groin hernia much less frequently. Epiploic appendages of the colon are considered to be one of the rarest types of such hernia content.
Case report: A 60 year male is brought to ER for severe pain in left inguinal region of several hours duration. Based on clinical history, physical examination findings of tender, irreducible lump at the left deep inguinal ring; along with leukocytosis, the patient was taken for emergency inguinal exploration. Findings of necrotic epiploica appendix adherent to normal sigmoid colon as the sole content of the hernial sac was surprising and indeed a rare event. A tension free mesh hernioplasty was accomplished.
Conclusion: Surprising hernial content as necrotic epiploica appendix may be encountered in clinical practice rarely, and can be managed with mesh repair if the wound is considered relatively clean.
Keywords
Necrotic epiploica; Inguinal hernia; Hernioplasty
Citation
Pangeni A, Rai S, Shakya VC, Byanjankar B (2017) Necrotic Epiploica Appendix as the Sole Content of Strangulated Inguinal Hernia. Ann Emerg Surg 2(3): 1013.
INTRODUCTION
It is well known that the most common content of a strangulated inguinal hernia is a small bowel loop or part of the major omentum [1]. Certain parts of the colon, urinary bladder, vermiform appendix, Meckel’s diverticulum, uterine tube and ovary, and other tissues may be observed in a strangulated groin hernia much less frequently [1]. Epiploic appendages of the colon are considered to be one of the rarest types of such hernia content [2].
This clinical situation (the strangulation of an epiploic appendage in an inguinal hernia) was described, independently and for the first time, by Serve and Muscatello in 1906, [3]. Likewise, we would like to present a similar but rare case of the strangulation and necrosis of an epiploic appendage of the sigmoid colon in a left indirect inguinal hernia.
CASE REPORT
A 60-year male who never had noticed a groin lump beforehand, is brought to emergency room with increasingly severe pain and a tender lump at left groin of 8-hour duration after a single event of harsh straining while working in the woods. The patient gives history of 2 episodes of projectile vomiting but denies obstipation or abdominal distension. The patient has no trauma to groin, pain in scrotum, negative for substance abuse except for cigarette smoking.
The patient was in understandable agony with a heart rate of 110 beats per minute, blood pressure of 160/60 mmHg supine, SpO2 96% in room air.
Examination, hindered by pain, of the Left groin revealed a tender, irreducible mass of 4X3cm in the left inguinal region. There were no skin changes.
A diagnosis of strangulated left inguinal hernia was made and patient shifted to operation theatre after hematological work up.
There was leukocytosis, total count 16,400 with neutrophilia. Rest of blood investigations was normal. X-ray abdomen showed no abnormality except for a loop of large bowel in left lower quadrant.
Under spinal anesthesia, left inguinal region was explored with a liberal incision over the swelling. An indirect inguinal hernial sac was dissected open to reveal small necrotic tissue covered by inflamed adipose elements. After suction and lavage of the area with normal saline, the sac of hernia was incised as to allow inspection of deeper structures.
It was revealed that the necrotic and hypertrophied tissue was the terminal part of an epiploica appendix attached to a normal sigmoid colon. The appendage was ligated at the base and removed, proper lavage done with Normal saline; and a tensionfree mesh repair was performed in usual manner.
The patient was discharged the next day. And on follow-up of 4th and 7th days he had no wound related complications.
DISCUSSION AND LITERATURE REVIEW
The intra-hernial torsion of an epiploic appendage was first presented for a femoral hernia by Riedel in 1905 and for an inguinal hernia separately by Serve and Muscatello in 1906 [3]. Although this variant of hernia content is rare [2,3], as early as 1919, Hunt surveyed 22 cases, in which an epiploic appendage was found in the hernia sac of a groin hernia, from the literature and added two cases from the Mayo Clinic [3]. Recently, certain case reports on this topic have been published [4-6], particularly with the addition of new imaging modalities for diagnosis. Most articles present the strangulation of a sigmoid epiploic appendage in a left inguinal hernia [4-7], and two with an extremely rare one in right inguinal hernia [8,9].
A wide range of recent actual problems are presented in this section: the possibility of preoperative diagnosis using modern imaging techniques; the choice of the operation extent; and indications for prosthetic groin hernioplasty in complicated hernias. In some above mentioned cases, the surgeons had to convert the approach to median laparotomy to allow the correct surgical incision for an obstructive sigmoid colon resection. Fortunately, in our case, the necrotic changes were limited to the epiploic appendage and were not extended to the bowel wall. We were able to correctly perform an operation using the primary left inguinal approach.

Figure 1: Findings at opening of sac.
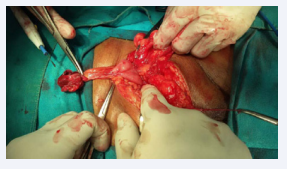
Figure 2: Necrotic Tip of appendix epiploica.

Figure 3: Friable necrotic tip of epiploica.
Finally, there are a few words about the chosen type of the hernioplasty. There has been a long and undulating debate on use of synthetic mesh in strangulated hernia. While it’s discouraged in frankly contaminated wounds, recent encouragements in use of mesh in most of strangulated cases can be attributed to work by various authors [10,11]. Elsabe et al., reported that, that excluded cases with frank peritonitis and resection, the use of mesh did not increase infection rates significantly whereas the rate of recurrence was low and concluded that use of Lichtenstein “tension-free” technique in emergency treatment of strangulated inguinal hernia is safe, effective with an acceptably low rate of postoperative complications and without recurrence [10]. Hentati et al., reviewed nine articles to conclude that the mesh repair technique is a good option for the treatment of strangulated inguinal hernias in adults, giving an acceptable wound infection rate and fewer recurrences than non-mesh repair [11]. We also did a tension-free mesh hernioplasty, ensuring that the remaining operative field was clean; and besides, the necrotic portion was only the tip of the appendage, and not the whole, and the infective load was relatively less; Our decision to put the mesh was right, and the recovery of the patient was uneventful without any postoperative wound infection.
CONCLUSION
Surprising hernial content as necrotic epiploica appendix may be encountered in clinical practice rarely, and can be managed with mesh repair if the wound is considered relatively clean.
REFERENCES
- VC Shakya, CS Agrawal, S Adhikary. A prospective study on clinical outcome of complicated external hernias. Health Renaissance. 2012: 10: 20-26.
- K Ballas, Th Kontoulis, Ch Skouras, A Triantafyllou, N Symeonidis, Th Pavlidis, et al. Unusual findings in inguinal hernia surgery: report of 6 rare cases. Hippokratia. 2009; 13: 169-171.
- VC Hunt. “Torsion of appendices epiploicae”. Annals of Surgery. 1919; 69: 31-46.
- Abdulzhavadov IM. Volvulus of the epiploic appendices of the sigmoid in strangulated inguinal hernia. Klin Med (Mosk). 1989; 67: 126-127.
- Ozkurt H, Karata? O, Karaarslan E, Ba?ak M. Clinical and CT findings of epiploic appendagitis within an inguinal hernia. Diagn Interv Radiol. 2007; 13: 23-25.
- Ozkurt H, Karatag O, Karaarslan E, Rozanes I, Basak M, Bavbek C. CT findings in epiploic appendagitis. Surgery. 2007; 141: 530-532.
- P. Klingenstein. Some phases of the pathology of the appendices epiploicae: with a report of four cases and a review of the literature. Surgery, Gynecology & Obstetrics. 1924; 38: 376-382.
- Shiryajev YN, Glebova AV, Chalenko MV. Strangulation and necrosis of an epiploic appendage of the sigmoid colon in a right inguinal hernia. Case Rep Surg. 2013; 2013: 890234.
- C. Bali, A. Tsironis, N. Zikos, M. Mouselimi, N. Katsamakis. An unusual case of a strangulated right inguinal hernia containing the sigmoid colon. Int J Surg Case Rep. 2011; 2: 53-55.
- Elsebae MM, Nasr M, Said M. Tension-free repair versus Bassini technique for strangulated inguinal hernia: A controlled randomized study. Int J Surg. 2008; 6: 302-305.
- Hentati H, Dougaz W, Dziri C. Mesh repair versus non-mesh repair for strangulated inguinal hernia: systematic review with meta-analysis. World J Surg. 2014; 38: 2784-2790.








































































































































