Non Operative Management of Traumatic Pneumopericardium: Case Report
- 1. Department of Cardiovascular Surgery, Institute for Cardiovascular Diseases C.C. Iliescu, Romania
Abstract
Pneumopericardium is a rare complication of blunt or penetrating chest trauma. GCS was 15. Simple penumopericardium can evolve to tension pneumopericardium with circulatory collapse. In this case, urgent drainage of the pericardial sac is mandatory. We present a case study of a 31 years old patient who presented with simple pneumpopericardium as a result of a chest stab wound. Due to his stable condition, we considered that non operative (conservative) management was the best strategy for this patient. This consists in intensive monitoring in intensive care for 24 hours and another 48 hours in critical care unit before being transferred in to a normal chamber, adequate pain control and antibiotic treatment. CT scan in the 5th day revealed no penumopericardium. Patient was discharged on the 7th day
Keywords
Pneumopericardium, Trauma, Non operative management
Citation
Robu M (2022) Non Operative Management of Traumatic Pneumopericardium: Case Report. Ann Emerg Surg 6(1): 1035.
INTRODUCTION
Pneumopericardium is defined as the presence of air within the pericardial space. It is a rare complication of blunt or penetrating chest trauma [1,2]. Simple pneumopericardium fallowing chest trauma does not produce any circulatory compromise but can evolve in tension pneumopericardium with circulatory collapse [3]. Management of tension pneumopericardium requires immediate drainage of the pericardial sac in order to achieve hemodynamic stability, preferable by a sub-xiphoid pericardial window (SPW) [4]. However, management of a simple pneumopericardium in a hemodynamic stable patient is more complicated. There are currently two strategies in the literature. First strategy is prophylactic decompression in order to prevent progression to tension penumopericardium. Second strategy is conservative and consists in monitoring the patient. The fallowing case study presents the non operative management of a simple traumatic pneumopericardium.
CASE REPORT
We present a case study of a 31 years old male admitted in the emergency department for chest trauma. GCS was 15. At the moment of admission in the emergency department, patient is hemodynamically and respiratory stable. Patient blood pressure was 147/100mmHg, regular heart rate at 100bpm, 100% O2 saturation, respiratory rate of 16/min, GCS E4,V5, M6, conscious. Physical examination reveals normal heart and lung sounds and a soft and non distended abdomen. Patient presents a 6 cm irregular subxifoid stab wound, with no active bleeding witch was sutured. Emergency transthoracic echography reveals no tamponade and normal function and dimensions of heart chambers. An emergency CT scan of the chest and abdomen revealed a substernal penetrating wound to the pericardium with pneumopercardium with no intrapericardial hematomas, no pneumothorax and no abdominal lesions (Figure 1a,b,c).
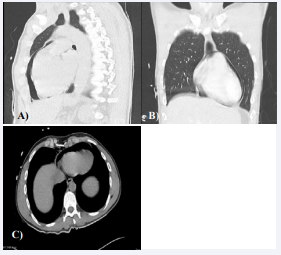
Figure 1: CT scan of the thorax showing pneumopericardium.
Patient remains stable, receives adequate pain control and antibiotics and is transferred in intensive care for monitoring. After 24h, patient remains stable and is transferred to cardiology ward for further surveillance. Patient rests for 48h in critical care unit before he is transferred to a normal chamber. Only pain medication and antibiotics are administrated. Transthoracic echography of the heart performed in day 2 reveals normal function and dimensions of the heart chambers, normal valves and no tamponade but this examination proves difficult to visualize any air in the pericardium. Patient remains stable and in the 5th day another CT scan of the thorax is performed. This examination reveals no pneumopericardium or pneumothorax and no mediastinal hematomas, false aneurisms or collections (Figure 2).
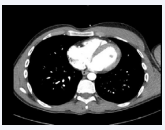
Figure 2: CT scan of the thorax on the 5th day of conservatory management showing absence of pneumopericardium.
Patient is discharged in the 7th day with normal evolution of the wound and no evidence of infection.
DISCUSSION
In the management of such a condition. The alternative is drainage of the pericardial space either percutaneous or surgically (SPW). In this case we preferred a non-surgical approach (conservative) with good end results. The main reason for this choice was the stable condition of the patient. Beside the pneumopericardium no other life-threatening conditions were associated. In this case conservative management eliminated the risk associated with invasive procedures such as SPW. In our opinion, the key when choosing this strategy is always considering the risk of progression from simple to tension penumoperitoneum. We recomand 24h surveillance in intensive care and at least 24-48h of surveillance on critical care unit before transferring the patient in to a normal chamber.








































































































































