Use of Treves Ileocaecal Fold for a Safe Laparoscopic Appendectomy
- 1. Department of Colorectal and General surgery, Southend University Hospital NHS Foundation Trust, UK
Abstract
Treves fold at ileocaecal junction remains an important landmark during laparoscopic appendectomy. Laparoscopic appendectomy has been deemed an acceptable substitute to an open surgery, though, an increased incidence of intra-abdominal infective complications have been reported. We have proposed an additional safety tip to otherwise well-known safe approach to laparoscopic appendectomy for junior doctors in training to avoid overzealous coagulation of mesoappendix contributing to immediate or delayed complications resulting from lateral thermal injury. We have validated this technique and have found it safe, reproducible and effective.
Keywords
Mesoappendix, Laparoscopic appendectomy, Treves ileocaecal fold, Vessel sealing devices, Safety
Citation
Bostan N, Jamalfar A, Jacob M (2016) Use of Treves Ileocaecal Fold for a Safe Laparoscopic Appendectomy. Ann Emerg Surg 1(1): 1002
ABBREVIATIONS
RCT: Randomized Controlled Trial; SAGES: Society of American Gastrointestinal and Endoscopic Surgeons
INTRODUCTION
The ileocaecal fold (bloodless fold of Treves) occupies the ileocaecal angle (Figure 1) and lies anterior to the mesoappendix. Its superior border is attached to antimesenteric border of terminal ileum; it’s inferior border on to the anterior surface of the mesoappendix, while the internal border is free and concave and forms the entrance to the ileocaecal fossa, which varies in depth and size. Treves fold has been well documented amongst anatomist but thus far no references have been made for its purpose as a landmark for a safe dissection in laparoscopic appendectomy.

Figure 1: Ileocaecal fold attached inferiorly to mesoappendix.
Laparoscopic appendectomy is one of the earliest and most common laparoscopic surgeries that have been performed safely by junior surgical trainees [1]. This short communication aims to provide an additional safety tip to an already well established safe and standardized technique in performing laparoscopic appendectomy by junior doctors. Treves ileocaecal fold has been considered as an important anatomical landmark to identify the ileocaecal junction and thereby locating appendix. Furthermore, it seems to retain a relatively constant property even in cases of complicated appendicitis (Figure 2,3), and therefore can be utilized with certainty to guide in locating the appendix as well as determining a safe dissection margin.
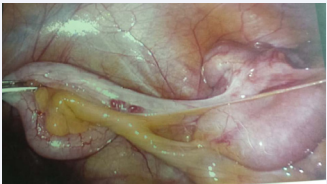
Figure 2a: Treves ileocaecal fold at laparoscopy in a thin female patient with normal appendix.
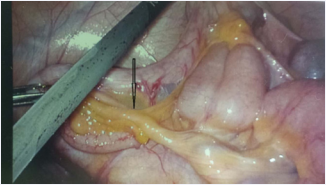
Figure 2b: Note the inferior attachment of fold to mesoappendix. Limiting coagulation of mesoappendix up to the attachment safeguards the blood supply to base of appendix and caecal pole.
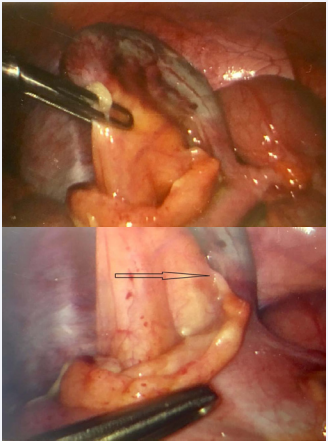
Figure 3: Prominent Treves fold with attachment to mesoappendix in an obese patient with complicated appendicitis. Limiting coagulation to the attachment (marked) ensures adequate blood supply to appendicular stump.
MATERIALS AND METHODS
Technique
Current evidence suggests that there is no particular technique that is superior in performing a laparoscopic appendectomy. Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) Guidelines for Laparoscopic Appendectomy (2009) concluded that developing a consistent method decreases costs, time, and complications [2,3]. Adhering to standard surgical principles is the best way to perform a safe laparoscopic appendectomy and includes creation of pneumoperitoneum by open technique, principles of triangulation in regards to trocar placement, and safe use of high energy sources. Readers should refer to above cited articles for further in-depth details.
As a supplement to above established guidelines, we have suggested use of diathermy to coagulate the mesoappendix only up to the attachment of Treves fold at mesoappendix. Any Figure 1 extensive coagulation beyond the attachment proximally leads to lateral thermal injury to ileal mesentery and beyond. This technique ensures preserving the proximal branches in the mesoappendix supplying caecal pole and appendicular stump (Figure 4).
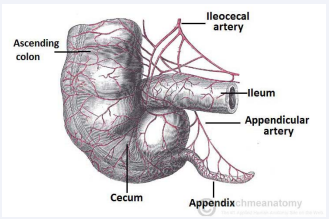
Figure 4: Blood supply to caecum and appendix; proximal mesoappendix containing branches to caecal pole and base of appendix.
It could be tempting to continue proximally aiming for the base of appendix especially in a thin patient (Figure 2)
Figure 2a: Treves ileocaecal fold at laparoscopy in a thin female patient with normal appendix.

Figure 2b: Note the inferior attachment of fold to mesoappendix. Limiting coagulation of mesoappendix up to the attachment safeguards the blood supply to base of appendix and caecal pole.
or in pediatric population. This safe technique has been validated at least in consecutive 50 patients, including cases of complicated appendicitis (Figure 3),
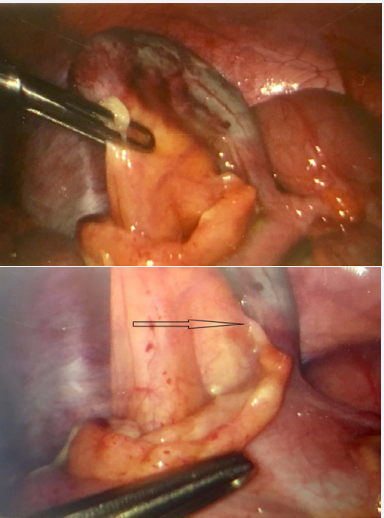
Figure 3: Prominent Treves fold with attachment to mesoappendix in an obese patient with complicated appendicitis. Limiting coagulation to the attachment (marked) ensures adequate blood supply to appendicular stump.
and found safe and reproducible amongst doctors in training.
RESULTS AND DISCUSSION
Appendicitis is a common surgical emergency. The lifetime incidence of appendicitis is 6 per cent and 70,000 appendectomies are carried out every year in the UK. In excess of 270 000 appendectomies are performed each year in the United States [4,5]. The 2002 National Confidential Enquiry into Patient Outcome and Death highlighted that appendicitis continues to carry a mortality rate, despite modern management. Although the majority of the mortalities was attributed by a diagnostic delay [6], the related post-procedural complications have been noted, which includes ongoing pain and inflammation around the appendicular stump or collection at right iliac fossa. Varying complications possibly from thermal injury have been postulated from late necrosis of bowel leading to intra-abdominal collection or fecal fistula.
While performing laparoscopic appendectomy various vessel sealing devices have been employed to coagulate mesoappendix before division. This includes monopolar diathermy, bipolar diathermy or sources like Harmonic scalpel or Ligasure by few. All except bipolar coagulation carries a risk of lateral thermal injury to adjacent ileal mesentery, small bowel or caecum leading to inadvertent injury directly or indirectly compromising the vascularity and subsequently presenting itself with delayed or late complications. To minimize this potential risk, Treves ileocaecal fold can be used as a guide to determine the extent of coagulation performed with assurance that the surgeon remains within the safe boundaries and not compromising the ileal mesentery.
The proportion of open procedures performed has fallen with the increased use of laparoscopic techniques. The Cochrane review included eight RCTs comparing laparoscopy with open appendectomy and revealed that laparoscopy resulted in more specific diagnosis especially in female population but there was no effect on the rate of adverse events [7]. Compared with open surgery, the systematic review found that laparoscopic appendectomy in adults reduces wound infections, postoperative pain, length of hospital stay, and time taken to return to work, although the number of intra-abdominal abscesses was higher after the laparoscopic approach [8]. This is supported further in a study by Kotaluoto and co-workers (2016) who found complications tends to be more severe with laparoscopic surgeries as compared to open appendectomies [9]. This could be the result of severity of appendicitis; however, we should try our best to minimize operative errors to the bare minimum by adhering to our proposed anatomical landmark for safe dissection in conjunction with already established standard surgical principles during laparoscopic surgery.
Future retrospective studies in correlating cases with postprocedural complications with analysis of intra-operative images for evaluating technique and extent of dissection margin may help to assess this further.
CONCLUSION
Treves fold at ileocaecal junction remains an important anatomical landmark during laparoscopic appendectomy in limiting extensive coagulation to mesoappendix and preventing lateral thermal injury. This technique is easily reproducible by the doctors in training and important in the era of laparoscopic appendectomy especially when coagulating with use of high energy sources.
ACKNOWLEDGEMENTS
The Bartleby.com edition of Gray’s Anatomy of the Human Body TeachMeAnatomy.info








































































































































