Joint Relations of Functionality, Socio-Demographic and Health Conditions in Institutionalized Elderly Individuals in Brazil
- 1. Federal University of Rio de Janeiro, Brazil
- 2. National School of Public Health/ Oswaldo Cruz Foundation, Brazil
Abstract
In the literature about health and ageing, there is a small number of investigations focusing socio-demographic and health characteristics of institutionalized older adults. This cross-sectional study aimed to analyze relationships between functionality, sociodemographic and health conditions in elderly individuals living in long stay institutions and to evaluate differences among residents living in cities of the Southeast and Middle West regions in Brazil. We used correspondence analysis to explore joint relationships between functionality limitations, socio-demographic conditions and health conditions and to identify the profile of the studied population. We surveyed 760 individuals, over half of which were male (52.6) while nearly 40.0% were 80 years old or older. Most of them showed dependence in instrumental activities of daily living (81.2) and cognitive deficit (73.3). We were able to identify three distinct profiles in the studied population. The group from Rio de Janeiro and Campo Grande was the youngest and healthiest; the group from Cuiabá was characterized by illiteracy and reading problems and comprised individuals with cognitive deficit and IADL-dependent and the last one (Juiz de Fora) comprised the oldest, most debilitated and least healthy individuals. This heterogeneity of profiles could be partially explained by sociodemographic and cultural contexts that lead to institutionalization of older adults in each city, indicating the possibility of different interventions aiming to prevent and reduce functional dependency, which would take into account specific features of targeted groups of elderly individuals.
Keywords
Elderly health , Long Stay Institutions for Elderly Individuals , Brazil
Citation
Santiago LM, do Carmo CN, Ferreira DB, Mattos IE (2014) Joint Relations of Functionality, Socio-Demographic and Health Conditions in Institutionalized Elderly Individuals in Brazil. Ann Gerontol Geriatric Res 1(4): 1019.
INTRODUCTION
In Brazil, long stay institutions for elderly individuals (LSIEI) consist of a type of care that provides collective housing to individuals aged 60 or older, with or without family support, and which may or may not be linked to a government initiative [1]. In general, these institutions provide health care and nutrition, social and religious services to its residents [2]. Such institutions “are different from hospitals, since they are collective households with living rules and operative logic, that varied according to their audience; sometimes they have elderly individuals with physical and/or cognitive problems under their care and, at other times, they function only as a home or shelter” [3]. Therefore, the LSIEI provide an alternative for individuals who are having trouble of self-managing and/or have insufficient income, for those without a family, for those whose family does not have the financial, physical and/or emotional means to provide necessary care to promote/maintain the elder’s wellbeing [4]. Unlike other countries, such institutions in Brazil usually have a permanent residence nature [2]. A large proportion of the elderly individuals in Brazil have lived under less privileged social and economic conditions and there is often no family caregiver to take responsibility for their health and survival [5]. As so, one of the demands arising from the ageing of Brazil’s population is the need for care in long stay institutions for elderly individuals (LSIEI). Although, several studies of elderly populations were conducted in this country, there are a small number of investigations addressing those that are institutionalized. Within that context, the aim of this study was to perform an analysis of the joint relationships between functionality, socio-demographic and health conditions in elderly individuals living in long stay institutions in order to evaluate the differences among LSIEI residents in four Brazilian cities.
MATERIAL AND METHODS
We conducted a cross-sectional study with residents of longstay institutions for elderly individuals in Rio de Janeiro and Juiz de Fora, in the Southeast region, and in Campo Grande and Cuiabá, in the Middle-West region, from September 2010 to February 2011. We chose to conduct this study across four cities based on the assumption that different socio-demographic, cultural and economic environments can influence the life histories and the way elderly individual’s age, with repercussions to their health conditions and functionality [6]. For the selection of the institutions included in the study, we opted to choose the biggest public LSIEI in each city. The selected LSIEI in Rio de Janeiro had a large number of residents as it is the only public institution in the city, but in the other cities the number of older adults was rather small. Because of it, we decided to select two more institutions in those cities in order to have a more balanced sample. The definition of older adult used in this investigation included individuals aged 60 or older, according to the Brazilian Senior Citizen Statute [7]. We assessed information for all individuals of that age, residing in the institution for at least 30 days from the date of the interview in each selected LSIEI. The study protocol was approved by the Committee of Ethics in Research of the National School of Public Health. Informed consent was provided by either the individuals themselves or by a legal representative of the institution if the individual was unable to sign on his/her own. The study population consisted of 760 institutionalized elderly individuals, distributed as follows: 254 (33.4%) in Rio de Janeiro, 193 (25.4%) in Juiz de Fora, 153 (20.1%) in Campo Grande and 160 (21.1%) in Cuiabá. The data collection instrument included socio-demographic variables, self-reported morbidity and selected health conditions assessed by instruments commonly used in evaluations of elderly populations. Functionality was assessed according to the Katz [8] and Lawton [9] scales. The first scale objectively assesses individual performance of Basic Activities of Daily Living (ADL), including six items (bathing, dressing, toileting, transferring to and from a bed or chair and feeding without help). Individuals who were unable to perform one or more activities without help were considered as ADL dependent [10,11]. Lawton’s scale targeting Instrumental Activities of Daily Living (IADL) assesses individual performance in the following activities: using the telephone; using transportation; shopping; taking medications on time; handling finances. We considered as IADL dependent those individuals who were unable to perform one or more activities without help [11-13]. The cut-off points utilized for the classification of ADL and IADL dependency were widely used in gerontology and geriatric literature in Brazil and other countries [10-14]. This tends to be a consensus, since the dependency in a single activity means that the older adult has not complete autonomy to execute his/hers social and functional role in its integrity. Cognition was assessed using the Mini-Mental State Examination (MMSE) [15], consisting of 20 questions that assess five aspects of cognitive functioning: spatial and temporal orientation, processing, attention, calculation, memory and language, totaling 30 points. Since the MMSE evaluation is influenced by one’s level of education, it is important to use cutoff points based on that variable in order to classify individuals according to test scores. We used 18/19 as cutoff points for elderly individuals without any education and 24/25 for individuals with any level of education. Lourenço and Veras suggested such cutoff points for use in the Brazilian elderly population [16]. In order to assess physical mobility, we used a group of questions from the data collection instrument of the Survey on Health, Well-Being, and Aging in Latin America and the Caribbean - SABE [17]. It consists of a set of twelve questions with four possible answers (no difficulty, some difficulty, great difficulty, unable to do it), which are addressed to the individuals or to their caregivers. Bedridden individuals were classified in a separate category that was not assessed for that condition. Depression symptoms were assessed using the Geriatric Depression Scale-15 (GDS-15), which enabled us to classify individuals into three categories, based on their total score: <5, no depression symptoms; 5-9, mild depression symptoms; and ≥ 10, severe depression symptoms [18]. With respect to sensory functions, we included questions that were also taken from the SABE survey [17] and which inquired about use of glasses or contact lenses and self-reported vision problems, use of hearing aid and questions addressing hearing problems. All the instruments used were validated for the Brazilian population [6,19-21]. Interviews and health examinations of the older adults were conducted by multidisciplinary teams, which were trained and standardized for every procedure.
DATA ANALYSIS
We performed a descriptive analysis of the study population of each city according to socio-demographic and health characteristics, using frequency distributions. In order to explore joint relationships between sociodemographic and health conditions and the functionality of institutionalized elderly individuals, and to establish the profile of the groups in the study population, we used correspondence analysis. To perform this analysis, we worked with the assumption that although institutionalized elderly individuals have a certain level of diversity with respect to their socio-economic level, we would be able to identify certain characteristics that were more related to the presence of functionality limitations. For this analysis, the following variables were selected: City where the institution is located (Rio de Janeiro, Campo Grande, Cuiabá and Juiz de Fora); Age group (60 to 69; 70 to 79; 80 and older); Level of education (illiterate; less than elementary school; elementary school; high school or above); Self-reported history of stroke (Yes/No); Self-reported history of cancer (Yes/No); Use of glasses or contacts (Yes/No); Feeling abandoned frequently (Yes/No); More memory problems than other people their age (Yes/No); Difficulty for walking 400 meters (no difficulty/with difficulty); MMSE temporal orientation score (0 and 1/2 and 3/4 and 5); difficulty in reading based on the MMSE (Yes/No); feeling of being frequently upset (Yes/No).
Multiple correspondence analysis (MCA) was used to study the set of associated factors, with the aim of reducing the dimensionality of features related to functionality (AVD and IADL). MCA is a multivariate, exploratory technique used to analyze categorical data in contingency tables. The technique uses a graphic visualization of associations between several categories of variables, identifying groups which have the same risk factors and which therefore are geometrically closer [22]. In order to obtain dimensions that would represent the configuration of categories of variables in space, we calculated a set of factor axes, each maximizing a part of the data’s variability [23]. Total inertia was the measurement we used to define the proportion of variability explained by each dimension. Total absolute inertia was decomposed into partial inertias for each dimension (relative inertias), which allowed us to find out how far total inertia could be explained by a given derived dimension. The statistical package Statistica, version 7 [24], was used to analyze data in this study.
RESULTS
The socio-demographic and health characteristics of elderly individuals can be seen in (Table 1). We notice a predominance of the male sex across all cities, except for Juiz de Fora. As for age, the exception was Rio de Janeiro, with more individuals aged 60- 79, while in other cities older individuals were predominant. In Middle West, cities over 50% of elderly individuals were illiterate, while 20 to 30% of individuals were illiterate in the Southeast. ADL dependency ranged from 42% (Rio de Janeiro and Cuiabá) to 60% (Campo Grande and Juiz de Fora). As for IADL dependency, the lowest prevalence was observed in Rio de Janeiro, with 76.8%, and the highest was observed in Cuiabá (86.9%). The prevalence of cognitive deficiency according to the MMSE was high (between 64.3% and 84.8%), with special notice to figures observed for elderly individuals in the Middle-West region. Depression symptoms were also significant, with prevalence ranging from 42.6% and 60.6%. As for self-reported morbidity, the diseases most often reported by elderly individuals were high blood pressure, cerebrovascular accidents, diabetes mellitus, joint conditions and cardiac disease.
Table 1: Socio-demographic and health conditions of the sample of elderly individuals living in long stay institutions in four Brazilian cities 2010- 2011.
| Variables | Southeast Region | Middle West Region | Total |
||
| Rio de Janeiro | Juiz de Fora | Campo Grande | Cuiabá | ||
| N (%) | N (%) | N (%) | N (%) | N (%) | |
| Sex | |||||
| Male | 150 (59.1) | 58 (30.1) | 90 (58.80) | 102(63.8) | 400(52.6) |
| Female | 104 (40.9) | 135 (69.9) | 63 (41.2) | 58 (36.3) | 360(47.4) |
| Age Group | |||||
| 60-69 years old | 74 (30.6) | 39 (20.4) | 35 (23.0) | 37 (23.1) | 185(24.8) |
| 70-79 years old | 101 (41.7) | 56 (29.3) | 55 (36.2) | 56 (35.0) | 268(36.0) |
| 80 years or older | 67 (27.7) | 96 (50.3) | 62 (40.8) | 67 (41.9) | 292(39.2) |
| Level of Education | |||||
| Illiterate | 45 (23.2) | 53 (29.9) | 69 (52.3) | 74 (52.9) | 241(37.5) |
| Less than Elementary School | 90 (46.4) | 53 (29.9) | 46 (34.8) | 44 (31.4) | 233(36.2) |
| Elementary School | 33 (17.0) | 33 (18.6) | 7 (5.3) | 9 (6.4) | 82 (12.8) |
| High School or above | 26 (13.4) | 38 (21.5) | 10 (7.6) | 13 (9.3) | 87 (13.5) |
| Reported Morbidity | |||||
| Hypertension* | 89 (48.4) | 51 (50.5) | 38 (54.3) | 42 (40.4) | 220(47.9) |
| Heart Disease* | 20 (11.0) | 27 (26.7) | 22 (32.4) | 9 (8.8) | 78 (17.2) |
| Stroke* | 19 (10.3) | 31 (30.7) | 12 (17.6) | 16 (15.5) | 78 (17.2) |
| Diabetes* | 34 (18.7) | 26 (25.7) | 14 (20.0) | 26 (25.7) | 96 (21.0) |
| Chronic Pulmonary Disease* | 10 (15.4) | 9 (8.9) | 14 (20.0) | 14 (13.6) | 47 (10.3) |
| Cancer* | 9 (5.0) | 1 (1.0) | 6 (8.7) | 3 (2.9) | 19 (4.2) |
| Joint Problems* | 29 (15.8) | 44 (43.6) | 15 (22.1) | 21 (20.2) | 109(23.9) |
| Psychiatric Diseases* | 32 (17.4) | 26 (25.7) | 11 (16.2) | 8 (7.8) | 77 (16.9) |
| Functional Capacity | |||||
| ADL dependency | 107 (42.1) | 114 (59.1) | 92 (60.1) | 68 (42.5) | 381(50.1) |
| IADL dependency | 195 (76.8) | 151 (78.2) | 132 (86.3) | 139(86.9) | 617(81.2) |
| Bedridden | 30 (11.8) | 23 (11.9) | 14(9.2) | 13 (8.1) | 80 (10.5) |
| Cognitive deficit | 117 (64.3) | 74 (74.0) | 58 (79.5) | 84 (84.8) | 333(73.3) |
| Depressive symptoms | 78 (42.6) | 63 (60.6) | 42 (57.5) | 45 (42.9) | 228(49.0) |
* Self-reported conditions
Table 2 shows the distribution of variables used in the multiple correspondence analysis, according to the presence of ADL and IADL dependency. In general terms, we observed: higher frequency of dependence among older individuals; that dependent elderly individuals tend to have little or no education; that they have trouble walking for 400 meters; that they do not report any reading problems; that they score low in the temporal orientation MMSE scale; and that they have no prior history of cerebrovascular accident. We also notice a diversity of frequencies in almost all co-variables, when they are separated according to the outcomes of interest of this study (chi-square test, p<0.05). This behavior was not verified only for the following variables: self-reported cancer, use of glasses or contacts, frequent feeling of abandonment and memory problems, among ADL-dependents.
Table 2: Distribution of dependents in Basic Activities of Daily Living (ADL) and/or Instrumental Activities of Daily Living (IADL) according to selected co-variables in the sample of elderly individuals living in Long Stay Institutions in four Brazilian cities 2010-2011.
| Variables |
ADL | IADL | ||||
| N | % | p-value* | N | % | p-value* | |
| City | ||||||
| Rio de Janeiro | 108 | 28.3 | 195 | 31.6 | ||
| Juiz de Fora | 114 | 29.8 | 0.00 | 151 | 24.5 | 0.02 |
| Campo Grande | 92 | 24.1 | 132 | 21.4 | ||
| Cuiabá | 68 | 17.8 | 139 | 22.5 | ||
| Age Group | ||||||
| 60 to 69 years | 67 | 18.0 | 131 | 21.8 | ||
| 70 to 79 years. | 126 | 33.8 | 0.00 | 217 | 36.0 | 0.00 |
| 80 years or older | 180 | 48.3 | 254 | 42.2 | ||
| Level of Education | ||||||
| Illiterate | 135 | 45.3 | 215 | 42.4 | ||
| Less than Elementary School | 89 | 29.9 | 0.00 | 179 | 35.3 | 0.00 |
| Elementary School | 35 | 11.7 | 54 | 10.7 | ||
| High School or above | 39 | 13.1 | 59 | 11.6 | ||
| Cancer | ||||||
| Yes | 10 | 6.4 | 0.15 | 19 | 5.8 | 0.02 |
| No | 147 | 93.6 | 306 | 94.2 | ||
| Stroke | ||||||
| Yes | 49 | 30.6 | 0.00 | 68 | 20.7 | 0.01 |
| No | 111 | 69.4 | 261 | 79.3 | ||
| Difficulty walking about 400 meters | ||||||
| No difficulty | 93 | 24.3 | 0.00 | 257 | 41.8 | 0.00 |
| Moderate difficulty | 289 | 75.7 | 358 | 58.2 | ||
| Temporal Orientation | ||||||
| 0 and 1 | 77 | 48.1 | 125 | 38.2 | ||
| 2 and 3 | 45 | 28.1 | 0.00 | 95 | 29.1 | 0.00 |
| 4 and 5 | 38 | 23.8 | 107 | 32.7 | ||
| Reading Problems | ||||||
| Yes | 60 | 37.3 | 0.04 | 120 | 36.4 | 0.00 |
| No | 101 | 62.7 | 210 | 63.6 | ||
| Frequently Annoyed | ||||||
| Yes | 82 | 50.3 | 0.04 | 156 | 46.8 | 0.03 |
| No | 81 | 49.7 | 177 | 53.2 | ||
| Wears glasses/contacts | ||||||
| Yes | 74 | 27.7 | 0.42 | 115 | 24.4 | 0.00 |
| No | 193 | 72.3 | 357 | 75.6 | ||
| Feeling of being abandoned | ||||||
| Yes | 63 | 38.7 | 0.31 | 136 | 40.8 | 0.00 |
| No | 100 | 61.3 | 197 | 59.2 | ||
| Memory problems | ||||||
| Yes | 37 | 22.8 | 0.64 | 80 | 24.2 | 0.03 |
| No | 125 | 77.2 | 251 | 75.8 | ||
*Chi-square test
Total absolute inertia was decomposed into partial inertias for each dimension (relative inertias), which allowed us to find out how far total inertia could be explained by a given derived dimension. We verified that the first two dimensions accounted for 22% of global variability (or total inertia) of data, while the first dimension accounts for 13%. Considering the absolute contributions of each variable for the composition of each factor, we noticed that elderly individuals who were not IADL-dependent, but were ADL-dependent, and had difficulty in walking 400 meters formed primarily the first axis. As for the second factor, the categories that contributed most for its formation were illiterate elderly individuals, with and without reading problems, who reported wearing glasses or contacts, and who reported a history of stroke.
Figure 1 shows a graphic representation of the categories of variables in the first factor plan, with two dimensions. Those two categories formed groups, which were selected based on a visual analysis of the graph generated by correspondence analysis. The groups were thus named:
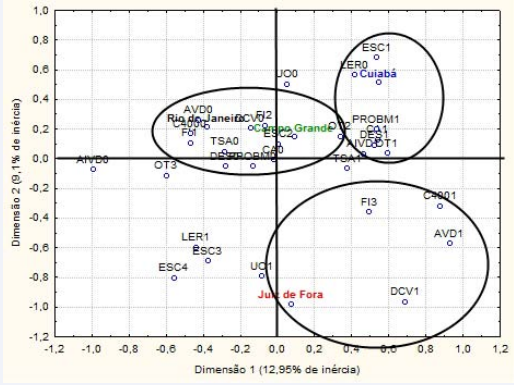
Figure 1 Graphic representation of the two first dimensions of the correspondence analysis in a sample of elderly individuals living in long stay institutions in four Brazilian cities 2010-2011. Caption: FI1: 60 to 69; FI2: 70 to 79; FI3: 80 and older; LER0: No Reading Problems; LER1: With Reading Problems; ESC1: Illiterate; ESC2: Less than Elementary School; ESC3: Elementary School; ESC4: High School or above; CA1: History of cancer; CA0: No history of cancer; DCV1: History of stroke; DCV0: No history of stroke; AVD0: No ADL dependency; ADL1: With ADL dependency; IADL0: No IADL dependency; IADL1: With IADL dependency; UO1: Wears glasses/contacts; UO0: Does not wear glasses/contacts; TSA0: Has not been upset recently; TSA1: Has been upset recently; DES0: Has not felt abandoned recently; DES1: Has felt abandoned recently; PROBM0: Has not had memory problems; PROBM1: Has had memory problems; C4000: No difficulty walking 400 meters; C4001: Difficulty walking 400 meters; OT1: Scored 0-1 in the temporal orientation scale; OT2: Scored 2-3 in the temporal orientation scale; OT3: Scored 4-5 in the temporal orientation scale.
Older adults from Rio de Janeiro and Campo Grande - those who were not ADL-dependent, who did not report having problems walking 400 meters, who did not feel upset often, who did not report memory problems, who did not feel abandoned and were aged 60 to 79 years.
Older adults from Cuiabá - those who reported reading problems, were illiterate, reported memory problems, felt abandoned, were IADL-dependent and scored 0 and/or 1 in the MMSE temporal orientation scale.
Older adults from Juiz de Fora - those who had difficulties to walk 400 meters, aged 80 years or older, were ADL-dependent and reported history of stroke.
DISCUSSION
In the national literature, there is a wide variation in the range of ages of institutionalized elderly individuals [2,5,25,26] and high illiteracy/low education rates [2,26,27]. The morbidities identified in our study are the most prevalent among institutionalized individuals from different regions in Brazil [2,5,26,28-30]. The high prevalence of functional incapacity in activities of daily living (ADL) and especially in instrumental activities of daily living (IADL) we observed among elderly individuals in this study confirms the findings of similar studies. Among elderly individuals from Frederico Westphalen (RS), 52.0% and 16.0% were partially and completely ADL-dependent, respectively, while 71.0% and 29% were partially and completely IADLdependent [5]. In a study conducted by Gonçalves et al (2010), 23.1% of the population was dependent with respect to at least one of the activities of daily living [27]. In a study conducted in Cuiabá (MT), it was also observed high prevalence of ADL (44.2%) and IADL (83.7%) dependency [26]. The relationship between advanced age and ADL/IADL dependency has been demonstrated in some studies conducted with elderly individuals who live in the community, although it has not been observed in others [13,14,31]. This association was also observed in studies with institutionalized elderly individuals [32,33]. Difficulty in walking interferes directly with the performance of activities of daily living, and its relationship with ADL dependency is understandable. In a Japanese study, the incidence of functional dependency was strongly associated with lower mobility [14]. Chronic diseases also contribute to functional dependency and high prevalence of those diseases has been observed among institutionalized individuals [33-36]. The relationship between level of education and/or cognitive deficit is well known in the literature [13,14,36-38]. In two studies with older adults in Japan, it was observed that low level of education was associated with cognitive deficit [14,36]. In other study, conducted with Brazilian elderly living in municipality of São Paulo the same was observed [13]. Due to the low level of education of the Brazilian elderly population, we should expect a high prevalence of cognitive deficit among institutionalized individuals, as well as of IADL dependency, since those activities require greater cognitive integrity. With respect to depressive symptoms, in a study conducted with elderly individuals in Japan and South Korea, high scores in a scale that assesses depression symptoms have been associated with decreased functioning ability [37]. Ageing, especially when accompanied by low functionality, may affect individuals’ self-esteem, leading to the onset of depressive symptoms. In the literature, demographic and socio-cultural variables have been associated with functional incapacity [11,13,31,33,38]. By exploring the joint relations between functionality, sociodemographic variables and health conditions, we were able to identify three different group profiles among the study population and to point out the characteristics most related to limitations, which were consistent with the literature. The group “Older adults from Rio de Janeiro and Campo Grande” was the youngest and healthiest group. They did not have any cognitive or mobility problems, as well as depression symptoms, and therefore had no functional dependency in ADLs. On the other hand, the group “Older adults from Cuiabá” was characterized by illiteracy and reading problems. It gathered individuals with cognitive deficit, such as a low scores in the temporal orientation scale, and IADL-dependent, interrelated aspects that in the literature are associated with education [11,13,31,33,38]. In this group, we also had individuals with depression symptoms, which may have emerged because of the IADL dependency as it imposes significant limitations to people’s independence [11,13,31,33,38]. This group was not characterized by a specific age range or by the presence of any morbidity. This led us to assume that this group was built on the very low level of education of those individuals. Finally, the group “Older adults from Juiz de Fora” comprised the oldest, most debilitated and least healthy individuals and, as expected, was characterized by ADL dependency. By exploring the joint relationships between functionality, socio-demographic and health conditions, we found great heterogeneity among the institutionalized elderly individuals in the studied cities. Therefore, this opens up new possibilities to think about interventions to prevent and reduce functional dependency, taking into account the particular characteristics of each specific group of older individuals, which we are targeting. Meanwhile, due to the socio-demographic and cultural diversity that exists among urban centers, it is necessary to exercise caution when generalizing the results of this study.
AUTHOR CONTRIBUTIONS
All authors participated equally throughout all stages of this study.
FINANCIAL SUPPORT
The INOVA ENSP 2010 Program of the National School of Public Health/Oswaldo Cruz Foundation funded the research project that originated this study.
REFERENCES
1. BRASIL. SEAS Secretaria de Ação Social. Portaria nº2874/2000. Instituições de Longa Permanência para Idosos (ILPI). Brasília: 2000.
3. Christophe M. Instituições de longa permanência para idosos no Brasil: uma opção de cuidados de longa duração? Dissertação (Mestrado) – Programa de Pós-Graduação em Estudos Populacionais e Pesquisas Sociais, Escola Nacional de Ciências Estatísticas, Rio de Janeiro, 2009, 178 f.
4. Instituto de Pesquisa Econômica Aplicada (IPEA). Características das instituições de longa permanência para idosos – região Sudeste/ coordenação geral Ana Amélia Camarano – Brasília: IPEA; Presidência da República, 2010. 242 p.
6. Marucci MFN, Barbosa AR: Estado nutricional e capacidade física. IN: Lebrão ML, Duarte YAO. SABE – Saúde, Bem-estar e Envelhecimento – O Projeto Sabe no município de São Paulo: uma abordagem inicial. Brasília: Organização Pan-Americana da Saúde, 2003.
7. BRASIL. Ministério da Saúde. Estatuto do idoso. Brasília: 2003.
24.Stasoft, Inc. Statistica (Data Analysis Software System), Version 7. Disponível em. 2004.









































































































































