Locally Advanced Castration Resistant Prostate Cancer Undetectable 114 Months after Short Course Palliative Radiotherapy: A Case Report
- 1. Division of Radiotherapy, ASST Valle Olona, Italy
Abstract
Introduction: In the last few years many new effective drug therapies have become available for the treatment of patients affected by castration-resistant prostate cancer such as new chemotherapies or second lines hormone therapies to addict to androgen deprivation therapy (ADT), while radiotherapy in this scenario is considered a palliative treatment only. We report an emblematic case.
Case Presentation: In June 2013, a 69 years old patient affected by castration resistant prostate cancer was referred to our department because of obstructive urinary symptoms. Serum prostate-specific antigen (PSA), was 33.32ng/ml, with a PSA doubling time (PSA-DT), of 1 month despite serum testosterone castration levels.
A radiolabelled [11C], choline positron emission tomography detected pelvic large disease only, with mesorectal and presacral lymph nodal metastases.
In July 2013, the patient underwent a palliative short course pelvic external beam radiotherapy (EBRT), 30Gy, 3Gy per fraction (5 fractions/week). One hundred and fourteen months after EBRT, the patient was alive, disease free, and with no obstructive urinary symptoms.
Discussion: The patients with non-metastatic castration resistant prostate cancer (NM-CRPC), with a short PSA-DT of ≤10 months are considered at high risk for the development of distant metastasis and should be treated with a second line hormonal therapy, with the addition of a modern antiandrogen to ADT until disease progression.
Long term androgen deprivation therapy causes many adverse effects and it impairs the quality of life.
According to our reported experience, EBRT could be a short-term, well-tolerated, low cost, effective treatment that should be taken into account in NM-CRPC
Keywords
Prostate cancer; Castration-resistant prostate cancer; Lymph node metastases; Radiotherapy
Citation
DE CICCO L, BORTOLATO B (2022) Locally Advanced Castration Resistant Prostate Cancer Undetectable 114 Months after Short Course Palliative Radiotherapy: A Case Report. Ann Mens Health Wellness 3(1): 1013.
ABBREVIATIONS
PSA: Prostate-Specific Antigen; PSA-DT: PSA Doubling Time; ADT: Androgen Deprivation Therapy; EBRT: External Beam Radiotherapy; CRPC: Castration-Resistant Prostate Cancer; NMCRPC: Non-Metastatic Castration Resistant Prostate Cancer; CT: Computed Tomography; PET: Positron Emission Tomography
INTRODUCTION
Prostate cancer is the second largest cancer diagnosis in men worldwide. Luteinising hormone-releasing hormone (LHRH), agonists or antagonists are the standard of care in the androgen deprivation therapy (ADT) [1]. A large number of patients are destined to develop a castration resistant disease.
In the last few years several new effective drug therapies have become available for treatment of patients affected by castrationresistant prostate cancer (CRPC), such as new chemotherapies or second lines hormone therapies (e.g. apalutamide, enzalutamide, abiraterone or darolutamide), while radiotherapy in this scenario is considered a palliative treatment only, even in the more recent guidelines [2]; there are limited data on the long-term outcomes on radiation treatments in this patient population.
Pelvic radiation treatment had showed a possible curative effect in a rate of patients affect by castration-resistant prostate cancer [3,4], even if large randomized study are lacking so that don’t exist evident selection criteria.
We experienced an emblematic case on this argument. We present a case of castration resistant, with very short PSA doubling time, locally advanced prostate cancer treated with short course external beam radiation therapy (EBRT), and disease free more than nine years later.
CASE PRESENTATION
In June 2013, a 69 years old patient affected by obstructive urinary symptoms because of a Gleason Score 4+4=8 prostate cancer in 14 out 14 cores at prostatic biopsy in July 2012, with an initial serum PSA 24ng/ml, suspicious bone metastases at bone scan and bladder invasion by a great pelvic mass at abdominal computed tomography (CT), scan at diagnosis. He was referred to our department after an early onset of total androgenic block resistance. The patient had underwent to hormonal therapy with Leuprorelina and Bicalutamide from July 2012 with a PSA nadir of 0.08ng/ml in October and a subsequent fast increase: 0.43 in November, 5.68ng/ml in February 2013, 10.27ng/ml in April, 26.88ng/ml in May, 33.32ng/ml at early July, with serum testosterone levels <20ng/dL, with a PSA doubling time (PSADT) from October 2012 to July 2013 of 1 month.
CT and magnetic resonance targeted excluded bony metastases; a radiolabelled [11C] Choline positron emission tomography (PET), detected pelvic disease only, with large mesorectal and presacral lymph nodal metastases (Figure 1).
![Figure 1 Pelvic tumor mass at the radiolabelled [11C]choline positron emission tomography](https://www.jscimedcentral.com/public/assets/images/uploads/image-1703144518-1.png)
Figure 1 Pelvic tumor mass at the radiolabelled [11C]choline positron emission tomography
A cystoscopy excluded mucosal involvement. Rectal digital examination detected a great fix hard pelvic mass anteriorly to the rectum.
After CT planning scan (Figure 2),
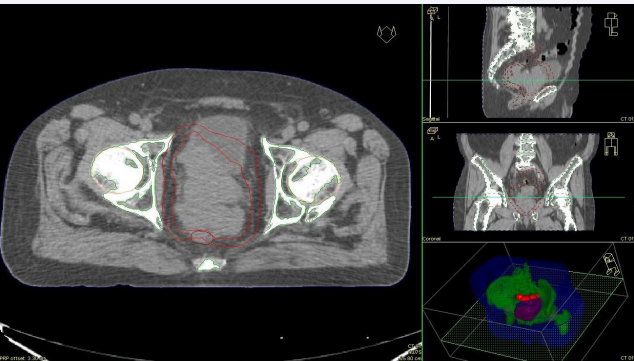
Figure 2 Pelvic radiation clinical target at the planning computed tomography
since pelvic disease size of about 250cc, and the high risk of microscopic distant metastases, a palliative short course EBRT directed to the PET positive disease was planned and performed in July 2013, with a total dose of 30Gy, 3Gy per fraction (5 fractions/week).
No radiation acute adverse effect was reported by the patient
One month later EBRT the PSA was 0.45ng/ml and from November 2013 to January 2015 PSA became undetectable (<0.03ng/ml). Obstructive urinary symptoms were improved and rectal digital examination showed a hypertrophic soft prostate.
Eighteen months after treatment delivering, hormonal therapy was stopped.
Six years after radiotherapy, a [11C] Choline PET-TC, planned because of a PSA bounce up to 8,15ng/ml, detected no residual disease (Figure 3).
![Figure 3 Axial pelvic computed tomography co-recorded to the radiolabelled [11C]choline positron emission tomography of 7 November 2019](https://www.jscimedcentral.com/public/assets/images/uploads/image-1703144764-1.png )
Figure 3 Axial pelvic computed tomography co-recorded to the radiolabelled [11C]choline positron emission tomography of 7 November 2019
Subsequently the PSA returned to stable serum levels around 1.5-2.2ng/ml up to the last follow up without any systemic therapy.
One hundred and fourteen months after treatment completion, the patient was alive, disease free, and in good health with no obstructive urinary symptoms. No late actinic adverse effect occurred during the follow up.
A written informed consent for patient information and images to be published was provided by the patient.
DISCUSSION
The patients with non-metastatic castration resistant prostate cancer (NM-CRPC) with a short PSA-DT of ≤10 months are considered at high risk for the development of distant metastasis and actually could be treated with a second line hormonal therapy, with the addition of a modern antiandrogen to ADT such as apalutamide, enzalutamide or darolutamide [1]. These treatments are usually continued chronically until disease progression.
Long term androgen deprivation therapy causes adverseeffects including bone loss, metabolic changes, gynecomastia, muscle loss, hot flashes, and possibly increased cardiovascular events, so that it impair health and quality of life [5]. According to literature, palliative pelvic radiotherapy for symptomatic castration resistant prostate cancer provides effective palliation of symptoms with acceptable toxicity [6]. White R et al, in a retrospective evaluation of a localized castration-resistant prostate cancer population treated with
palliative intent radiotherapy, with no evidence of regional or distant disease, and who received a local well tolerated radiotherapy at dose equivalent to 40 Gy or greater, reported a high rate of local control; some patients had extended survival without evidence of disease progression [3].
According to Aizawa R et al., who reported on a 31 NM-CRPC patients series treated with definitive EBRT, with a median prostate dose of 70.4 Gy, a long-term disease-free and clinical failure-free status were reached in approximately one-third of and half of the treated patients, respectively; this approach was also associated with favorable local relapse-free rates and overall survival outcomes [7].
Definitive EBRT is a possible approach for NM-CRPC patients.
In our case, a relatively low dose well tolerated EBRT with palliative intent was enough to eradicate a large pelvic tumor mass.
According to our reported experience, radiotherapy could be a short-term, well-tolerated, low cost, effective treatment that should be taken into account in NM-CRPC.
DECLARATIONS
Conflict of Interest
The authors declare no financial interest and no conflict of interest.








































































































































