Comparison of Personality Disorders during Three Decades (1920–1929 vs 1930-1939 vs. 2000-2009) in Psychiatric Hospital Vrapce Croatia
- 1. Psychiatry and psychotherapy clinic “Furtbachkrankenhaus”, Germany
Abstract
Aim: To compare demographic characteristics, comorbidities and diagnoses of patients admitted to the Psychiatric Hospital Vrap?e for personality disorders during three decades 1920-1929, 1930-1939 and 2000-2009.
Methods: Data was collected from the archives for a 30-year period, from January 1920 to December 1939 and from January 2000 to December 2009. We used several definitions of personality disorders: Prichard’s concept of moral insanity, Koch’s concept of psychopathy, Schneider’s classification of psychopathy and the unpublished definitions of one of the hospital’s superintendents. For the period from 2000 to 2009 we used DSM-IV and ICD-10 as classification systems.
Results: The total number of admissions as well as the number and percentage of admissions discharged with a diagnosis of personality disorder continually increased. The maximum number of readmissions increased in the period from 2000 until 2009. Most of the patients were male and the average age at admission increased. The percentage of patients who were divorced, unemployed and retired increased whereas the percentage of patients widowed, employed and of those sent to the hospital by courts and police decreased. During the twenties there were 10 different terms and during the thirties 20 different terms used for personality disorders with Psychopathy being the most frequent term in both periods. From 2000 until 2009 there were 12 different terms for personality disorders with Emotionally unstable personality disorder being the most frequent one.
Conclusion: Most of the parameters describing personality disorders have significantly changed over time. More historical and medical studies are needed in order to compare the differences found in our study.
Keywords
Epidemiology; Personality disorders; Inpatients; Systematized nomenclature of medicine; History of medicine
Citation
Paštar Z (2017) Comparison of Personality Disorders during Three Decades (1920–1929 vs. 1930-1939 vs. 2000-2009) in Psychiatric Hospital Vrapce, Croatia. Ann Neurodegener Dis 2(1): 1020.
INTRODUCTION
Personality disorders represent extreme or significant deviations from the way in which the average individual in a given culture perceives, thinks, feels and relates to others [1,2]. Abnormal personality traits exist in milder forms in normal individuals, but if the traits manifest themselves as inflexible responses to a broad range of personal and social situations and result in considerable personal distress or social disruption, this condition is called personality disorder [3]. There are no pathognomonic symptoms for personality disorders as are, for example, psychotic symptoms in schizophrenia or dysregulation of mood in affective disorders. Persons with personality disorders are pathognomonic as a whole personality in relation to others, so to understand personality disorders it is necessary to understand not only the person with the personality disorder but also the culture in which that person lives. It is quite obvious that differences in culture exist geographically, but they also exist historically. Every time period has to be looked at in a context of its own, with its own ‘’rules’’, specific way of thinking, and norms in terms of expected behavior. As it is characteristic of personality disorders to «break these rules», investigating the history of the development of the concept of personality disorders is not only academically important but it also sheds light on a broad field of social factors that are essential in diagnosing personality disorders. This is all the more important given that previous researchers have shown that there is no firm biological bases for the development of personality disorders [4-9]. On the other hand, there are more and more studies of possible connection between biological parameters and the development of personality disorders. Following parameters have been shown as relevant for the development of personality disorders: Diabetes and insulin resistance [10-14], Magnesium therapy, diet and nutrition [12,13], increased xenobiotics in the food, water and air [15,16]. There is an open discussion about the possible connection between chronic diseases and personality disorders [11]. Among other factors connected to personality disorders, it is worth to mention that the personality disorders are differently connected withhomicide in developing and in developed countries like Croatia [17,18].
In the Psychiatric Hospital Vrap?e, in Croatia, it is possible to conduct historical and medical research of personality disorders because Vrap?e Psychiatric Hospital contains archives with medical documentation on all patients treated in the hospital from its founding year in 1879 [19]. This study analyzed the development of nomenclature for personality disorders, they’re comorbidities, the ratio between admissions of personality disorders and total number of admissions, demographic characteristics of patients with personality disorder, such as sex, age distribution, marital status and employment, the ratio of patient with the diagnosis of personality disorder sent to hospital by court or police compared to the total number of patients with personality disorders and finally analysis of the length of stay in hospital. The only period investigated until now, in such a way, was from the hospitals founding year in 1879 until 1929 [19]. That study showed that the archives of the Psychiatric Hospital Vrap?e contain reliable data about the earliest patients with personality disorders [19]. In our study we investigated the same parameters but for the ten year period following, from 1930 and 1939 so that a comparison of parameters for the two subsequent time periods could be made. Additionally we investigated the same parameters in a recent time period, from 2000 to 2009 so that we could explore differences for the two not subsequent time periods (1930 – 1939 vs 2000 – 2009).
Vrap?ePsychiatric hospital between 1930 and 1939 with description of medical records
During the period between 1930 and 1939 the hospital superintendent was Dr Rudolf Herceg. He was a student of dr Ivo Žirov?i? who was one of the most prominent hospital superintendents in the history of the hospital and whose contributions in the field of forensic psychiatry and psychiatric classification had significant impact on the very foundation of Croatian psychiatry. Following the ideas of Dr Žirov?i?, Dr Herceg continued to work on the development of the hospital. In 1933 the hospital opened a new ward, one for somatic diseases, during that same period the first school for paramedics in the whole state also opened. The hospitals capacity further increased with the opening of a new department a few kilometers away from the hospital Vrap?e, called Jankomir. Later, in 1958, Jankomir became a separate psychiatric hospital. During the thirties insulin coma treatment and cardiazol were introduced. The name of the hospital changed from the National institute for the insane to the Hospital for mental illnesses. Thus, the thirties were a «golden age» for Vrap?e Psychiatric Hospital.
The medical records in the thirties compared to those in 1879 did not significantly differ in terms of general appearance, paper dimension (36 cm x 22.5 cm), and general patient data on the cover page [19]. Significant differences exist in the content of the medical records. First, during the thirties blood samples for every patient were submitted for serological testing according to Wasserman (diagnostics of syphilis) among other blood tests, every patient also underwent a lumbar puncture. Second, after the year 1935 medical records included detailed reports on insulin induced comas, with data regarding doses of insulin applied and the neuro-somatic reactions of patients to the applied insulin. Interestingly, after the year 1935 the majority of patients with personality disorders received insulin induced coma treatment. Third, much of the text in the medical records was written with a typewriter. Fourth, during the thirties there was a lot more additional documentation, including court records, detailed heteroanamnestic data. Documents describing the reason the patient was sent to hospital were structured, unlike in 1879. These documents also contained data pertaining to family history of illnesses, somatic illnesses of the patient, functioning at work and the social conditions of the patient [19]. The Fifth difference is very interesting. During 1879, the text was written partially in Croatian and partially in German. From 1930 until 1939, the text was partially written in Latin Croatian and partially in the Serbian Cyrillic alphabet. This was in concordance to the different political systems that Croatia was a part of, in 1879 Croatia was part of the Austro-Hungarian monarchy and during 1930 and 1939 Croatia was part of the Yugoslavian kingdom with the capitol city being Belgrade, Serbia. The medical records during the third observed period, from 2000 until 2009 were written completely in Croatian. This finding is a small indicator of the turbulent, but glorious history of Croatia.
MATERIALS AND METHODS
This study is a retrospective, cross-sectional study of medical records at the Vrap?e Psychiatric Hospital. In the examined period, all admissions were taken into account, even readmissions of the same patient. The relevant diagnoses were those listed at discharge. Comorbidity was defined as the presence of one or more illness (diagnoses) in addition to personality disorder [20- 22]. We investigated a 30 year period, from January 1, 1920 to December 31, 1939 and from January 1, 2000 to December 31, 2009. Data for the period from January 1, 1920 to December 31, 1929 was obtained from our previous research of the period from November 15, 1879 to December 31, 1929 [19]. First we compared the data for the period between January 1, 1920 to December 31, 1929 to the data for the period between January 1, 1930 to December 31, 1939. Next we compared the period from January 1, 1930 to December 31, 1939 and the period from January 1, 2000 to December 31, 2009.
The records
According to the 10-th edition of the International Classification of Diseases (ICD-10), personality disorders are placed in a diagnostic category with the code F60. According to the 4-th edition of Diagnostic and statistical manual of mental disorders (DSM-IV) the category of personality disorders includes the schizotypal personality disorder which is in a different category, under the code F21, in ICD-10. All admissions with a discharge diagnosis belonging to the current diagnostic category of personality disorders F60 and schizotypal personality disorder F21 were included in the analysis [1,2]. We used Prichards concept of Moral Insanity from 1835 [23-25], Koch’s concept of psychopathic inferiority from 1891 [26].
Schneider’s classification of psychopathic personalities from the year 1923 [3,27], and unpublished classification of Aleksej Kužljenko, MD who was hospital superintendent between 1929 and 1930 to determine the diagnosis of personality disorder in the period between 1920 and 1939.
Only the data that was complete and readable was taken into consideration. During the investigated time period between 1920 and 1939 and between 2000 and 2009 the following parameters were analyzed for personality disorders: the number of admissions with a discharge diagnosis of personality disorder was compared with the total number of admissions, distribution according to sex, average age, marital status (single, married, divorced, widowed), employment (employed, unemployed, retired), number of admissions with a diagnosis of personality disorder sent by courts or police, and the average length of hospital stay. We also explored the maximum number of readmissions per each patient. The nomenclature of all diagnoses of personality disorder and comorbidity was noted.
Statistical analysis
The median and interquartile range was reported for continuous variables, because of their asymmetric distribution. Nominal variables were analyzed with the Pearson χ2 test. Statistical significance level was set at P<0.05. Statistical analysis was carried out using SPSS for Windows, version 13.0 (SPSS Inc., Chicago, IL; USA) and Microsoft Excel, version 11 (Microsoft, Redmond, WA, USA).
RESULTS
Analysis of patients diagnosed with personality disorder
Our previous research showed that the total number of admissions to the Vrap?e Psychiatric Hospital during the period between 1879 and 1929 was 18,960. During the last ten years of that period, between 1920 and 1929, there were 7,514 total admissions, 135 of these admissions were discharged with a diagnosis of personality disorder (1.79%). Between 1930 and 1939 there were 8,355 total admissions of which 197 admissions were discharged with a diagnosis of personality disorder (2.36%) and between 2000 and 2009 there were 75,386 total admissions, 7,514 of these were discharged with a diagnosis of personality disorder (9.97%) (χ2=916,319; df=2; P<0,001). In considering the maximum number of readmissions we found that during the twenties one patient was discharged from the hospital 6 times with the diagnosis of a personality disorder, during the thirties the maximum number of readmissions for a patient was 5, and between 2000 and 2009 there was one patient who was admitted to the hospital 95 times and discharged each time with a diagnosis of personality disorder (χ2=151,151; df=2; P<0,001) (Table 1).
Table 1: Total number of admissions, number and percentages of admissions with the discharge diagnosis of personality disorder and maximum number of readmissions compared between three investigated decades.
|
|
1920-1929 |
1930-1939 |
2000-2009 |
|
Total number of admissions |
7,514 |
8,355 |
75,386 |
|
Number of admissions with the discharge diagnosis of personality disorder (%) |
135 (1.79%) |
197 (2.36%) |
7,514 (9.97%) * |
|
Maximum number of readmissions per patient with the discharge diagnosis of personality disorder |
6 |
5 |
95 * |
|
* χ2test |
|||
Therefore, during the thirties there was an 11.19% increase in the total number of admissions in comparison to the twenties, as for the period between 2000 and 2009 there was more than a tenfold increase in the total number of admissions in comparison to the period between 1930 and 1939. When considering the number of admissions with the discharge diagnosis of personality disorder, in the thirties there was an almost 0.5-fold (45.92%) increase in the number of these admissions when compared to the twenties, and during the period between 2000 and 2009 there was more than a 38-fold increase in comparison to the period between 1930 and 1939.
We found that during the thirties the proportion of admissions with a personality disorder increased more than 1.3- fold compared to the twenties, and between 2000 and 2009, there was more than a 4-fold increase in this proportion in comparison to the thirties. When considering the percentage of patients admitted with personality disorders during each ten year period there was a decrease during the twenties from 2.97% in 1920 to 1.17% in 1929. During the thirties the percentage increased from 1.33% in 1930 to 3.82% in 1939, and in the period between 2000 and 2009 the percentage slightly increased from 10.36% in 2000 to 10.60% in 2009 (Figure 1).
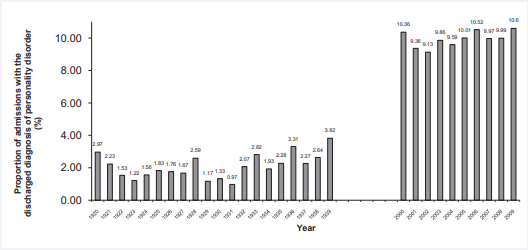
Figure 1: Percentages of admissions with the discharged diagnosis of personality disorder between 1920 and 1939 compared to the same percentages between 2000 and 2009.
If we consider the maximum number of readmissions per one patient, during the thirties this number was less then in the twenties (6 readmissions during the twenties, 5 readmissions during the thirties). During the period between 2000 and 2009, the maximum number of readmissions per one patient increased 19-fold in comparison to the thirties (5 readmissions during the thirties, 95 readmissions during the period between 2000 and 2009).
The characteristics of patients discharged with a diagnosis of personality disorder were significantly different in almost every investigated parameter. We would like to emphasize that during the investigated periods (1920-1929, 1930-1939, 2000- 2009) the average age of patients diagnosed with a personality disorder increased with time (median years: 28, 30, 40), more patients were divorced (percentage: 0%, 1%, 22.7%), unemployed (percentage: 14.2%, 9.6%, 53.8%) and retired (percentage: 0%, 0.5%, 21.2%). Fewer patients were employed (percentage: 85.8%, 89.9%, 25%), the average length of stay in hospital decreased (median days: 92, 80, 10) and the percentage of patients which were sent to the hospital by courts or police also decreased with time (62.9%, 15.7%, 1.3%) (Table 2).
Table 2: Admitted patients compared according to the demographic characteristics, proportion of those sent by courts or police and according to the length of stay in hospital between three investigated decades.
|
Characteristics |
Number (percentage) of admissions with the discharge diagnosis of personality disorder |
|
|
||
|
1920 – 1929 |
1930 – 1939 |
2000 – 2009 |
χ2 test |
P |
|
|
Sex, No.(%) male female |
115 (85.2) 20 (14.8) |
112 (56.8) 85 (43.2) |
5235 (69.7) 2279 (30.3) |
30,652 |
<0,001 |
|
Marital status, No.(%) married single widowed divorced |
40 (29.9) 81 (60.4) 13 (9.7) 0 |
49 (24.9) 139 (70.5) 7 (3.6) 2 (1) |
2360 (31.4) 3257 (43.3) 193 (2.6) 1704 (22.7) |
139,046 |
<0,001 |
|
Employment, No.(%) employed unemployed retired |
115 (85.8) 19 (14.2) 0 |
177 (89.9) 19 (9.6) 1 (0.5) |
1881 (25) 4044 (53.8) 1589 (21.2) |
634,921 |
<0,001 |
|
Sent to the hospital by courts or police, No. (%) |
85 (62.9) |
31 (15.7) |
98 (1.3) |
35,393 |
<0,001 |
|
|
Median years and median length of stay in hospital of admitted patients with the discharge diagnosis of personality disorder |
Kruskal-Wallis test |
P |
||
|
1920-1929 |
1930-1939 |
2000-2009 |
|||
|
Age, median years (interquartile range) |
28.00 (28.00-14.00) |
30.00 (30.00-16.00) |
40.00 (40.00-18.00) |
200,184 |
<0,001 |
|
Median length of stay in hospital, median days (interquartile range) |
92.00 (92.00-132.00) |
80.00 (80.00-142.00) |
10.00 (10.00-24.00) |
581,404 |
<0,001 |
In Vrap?ePsyhiatric hospital there were 685 admissions following court or police intervention, between 2000 and 2009, 98 (14.31%) of these admissions were diagnosed as personality disorders. These 98 admissions represent 1.3% of all admissions with the diagnosis of personality disorder, as shown in table (2).
Comparison of personality disorder nomenclature
During the twenties there were ten different terms for personality disorders, the most frequent term was Psychopathy followed by Psychopathic inferiority, Psihopathia post epileptica, Psychopathy with ethical defects and Psychopathia shizoides (Table 3).
Table 3: Terms used for personality disorders in patients admitted to Psychiatric Hospital Vrap?e and the number of associated admissions between 1920 and 1929.
|
Personality disorders between 1920 and 1929 |
|
|
Term |
No.of admissions |
|
Psychopathy |
122 |
|
Psychopathic inferiority |
2 |
|
Psihopathiapostepileptica |
2 |
|
Psychopathy with ethical defects |
2 |
|
Psychopathiashizoides |
2 |
|
Psychopathic stupor |
1 |
|
Psychopathy with hysterical traits |
1 |
|
Pathological affect – Psychopathy |
1 |
|
Psychopathia, sine morbopsychico |
1 |
|
Psihopathia gravis |
1 |
During the thirties there were 20 different terms for personality disorders. One patient, in 1932, had more than one diagnosis of personality disorder (Psychopathy and Hypomanic temperament). Like in the twenties, the most frequent term used for personality disorders was Psychopathy followed by the terms Psychopathia shizoides, Psychopathia epileptoides, Psychopathiaparanoides, Paranoid personality, Psychopathy with hysterical traits and Hypomanic psychopathy (Table 4).
Table 4: Terms used for personality disorders in patients admitted to Psychiatric Hospital Vrap?e between 1930 and 1939. Due to the fact that one patient had more than one diagnosis of personality disorder, the data for personality disorders in table 4 is expressed in the number of diagnosis
|
Personality disorders between 1930 and 1939 |
|
|
Term |
No. of diagnosis |
|
Psychopathy |
158 |
|
Psychopathiashizoides |
13 |
|
Psychopathiaepileptoides |
4 |
|
Psychopathiaparanoides |
4 |
|
Paranoid personality |
3 |
|
Psychopathy with hysterical traits |
2 |
|
Hypomanic psychopathy |
2 |
|
Moral Insanity |
1 |
|
Epileptoid-degenerative type of psychopathy |
1 |
|
Psychopathia gravis |
1 |
|
Psychopathia levis |
1 |
|
Paranoid personality with explosive character |
1 |
|
Manic psychopathy |
1 |
|
Childrens and adolescent psychopathy |
1 |
|
Psychopathy with homosexual drive |
1 |
|
Psychopathiashizoides, degenerative type |
1 |
|
Mixed shizoid and paranoid psyhopathy |
1 |
|
Psychopathic state |
1 |
|
Psychopathic constitution |
1 |
|
Hypomanic temperament |
1 |
Between 2000 and 2009 there were 12 different terms for personality disorders. The most frequent diagnosed personality disorder was emotionally unstable personality disorder – F60.3 (26.6%), followed by Dissocial personality disorder – F60.2 (24.2%) and Other personality disorder – F60.8 (18.3%). The least frequent diagnosis of personality disorder was anancastic personality disorder – F60.5 (0.3%) (Table 5). In this period 42 admissions were diagnosed with more than one personality disorder.
Table 5: Terms used for personality disorders in patients admitted to Psychiatric Hospital Vrap?e between 2000 and 2009. Due to the fact that 42 admissions were diagnosed with more than one personality disorder.
|
Personality disorders between 2000 and 2009 |
|
|
Term (code) |
No. of diagnosis (%) |
|
Emotionally unstable personality disorder (F60.3) |
1999 (26.6) |
|
Dissocial personality disorder (F60.2) |
1829 (24.2) |
|
Other personality disorder (F60.8) |
1384 (18.3) |
|
Dependent personality disorder (F60.7) |
520 (6.9) |
|
Personality disorder, Unspecified (F60.9) |
490 (6.5) |
|
Shizotypal personality disorder (F21) |
372 (4.9) |
|
Histrionic personality disorder (F60.4) |
253 (3.3) |
|
Personality disorder (F60) |
287 (3.8) |
|
Paranoid personality disorder (F60.0) |
214 (2.8) |
|
Shizoid personality disorder (F60.1) |
108 (1.4) |
|
Anxious (avoidant) personality disorder (F60.6) |
78 (1) |
|
Anankastic personality disorder (F60.5) |
21 (0.3) |
Comparation of comorbidity
During the twenties there were 135 admissions with the discharge diagnosis of personality disorder. 103 (76.3%) out of 135 were discharged with a single diagnosis of personality disorder. The remaining 32 (23.7%) were discharged with one or more comorbid diagnosis. The most frequent comorbid diagnosis was Ganser syndrome (prison psychosis), followed by chronic alcoholism, pathological intoxication with alcohol and cocainism (Table 6).
Table 6: Terms of comorbid diagnoses between 1920 and 1929 with the associated number of admissions.
|
Comorbidity between 1920 and 1929 |
|
|
Term |
No. of admissions |
|
Ganser syndrome (prison psychosis) |
12 |
|
Chronic alcoholism |
5 |
|
Pathological intoxication with alcohol |
3 |
|
Cocainism |
2 |
|
Lysteriform stupor |
1 |
|
Hysteric stupor |
1 |
|
Hysterical twilight state |
1 |
|
Alcoholic twilight state |
1 |
|
Surditas (deafness) |
1 |
|
Meningo-encephalitis circumscriptachronica |
1 |
|
Dipsomania |
1 |
|
Mental retardation |
1 |
|
Alcoholism |
1 |
|
Epilepsy |
1 |
During the thirties there were 197 admissions with the discharge diagnosis of personality disorder. 158 (80.2%) out of 197 were discharged with a single diagnosis of personality disorder. The remaining 39 (19.8%) were discharged with one or more comorbid diagnosis. The most frequent comorbid diagnosis was Alcoholism, followed by Mental retardation, Chronic alcoholism, Morphinism, Reactive depression and Morphinismuschronicus (Table 7).
Table 7: Comorbidity between 1930 and 1939 with the associated number of admissions.
|
Comorbidity between 1930 and 1939 |
|
|
Term |
No. of admissions |
|
Alcoholism |
15 |
|
Mental retardation |
5 |
|
Chronic alcoholism |
3 |
|
Morphinism |
3 |
|
Reactive depression |
2 |
|
Morphinismuschronicus |
2 |
|
Menopause |
1 |
|
Hypomania |
1 |
|
Hysteria |
1 |
|
Pulmonary tuberculosis |
1 |
|
Hypomanic state |
1 |
|
Mania |
1 |
|
Ganser syndrome (prison psychosis) |
1 |
|
Degenerative psychosis |
1 |
|
Hypomanic temperament |
1 |
One patient was given the diagnosis of Psychopathy with a comorbid diagnosis also belonging to the category of personality disorders, namely Hypomanic temperament. In the thirties Gansers psychosis was one of the least frequent comorbid diagnosis, unlike during the twenties when this was the most common comorbid diagnosis.
Between 2000 and 2009 there were 7,514 admissions with the discharge diagnosis of personality disorder. Among them there were 722 (9.6%) admissions with no comorbidity, i.e having only a diagnosis of personality disorder. The remaining 6,792 (90.4%) admissions had one or more comorbid diagnosis. These 6,792 admissions were diagnosed with a comorbid diagnosis for 10,184 times which means that these admissions have an average of 1.5 comorbid diagnosis. The most frequent comorbidity belonged to the diagnostic group of Mental and behavioral disorders (F00-F99) (90.7%), followed by External cause of morbidity and mortality (V01-X-Y98) (2.48%), Diseases of digestive system (K00-K93) (2.24%) and Diseases of nervous system (G00-G99) (1.66%) (Table 8).
Table 8: Comorbidity between 2000 and 2009 expressed in the number (percentages) of times diagnosed as comorbid diagnosis among the admitted patients with the comorbidity.
|
Comorbidity between 2000 and 2009 |
|
|
Group of diagnosis according to ICD-10 classification |
No. of diagnosis (%) |
|
Mental and behavioural disorders (F00-F99) |
9236 (90.70) |
|
External causes of morbidity and mortality (V01-X-Y98) |
253 (2.48) |
|
Diseases of the digestive system (K00-K93) |
228 (2.24) |
|
Diseases of nervous system (G00-G99) |
169 (1.66) |
|
Endocrine, nutritional and metabolic diseases (E00-E90) |
91 (0.89) |
|
Diseases of the circulatory system (I00-I99) |
70 (0.69) |
|
Injury, poisoning and certain other consequences of external causes (S00-T98) |
37 (0.36) |
|
Infectious and parasitic diseases (A00-B99) |
28 (0.27) |
|
Diseases of the respiratory system (J00-J99) |
25 (0.24) |
|
Factors influencing helath status and contact with helath services (Z00-Z99) |
8 (0.08) |
|
Diseases of the blood and blood-forming organs and disorders involving the immune mechanism (D50-D89) |
8 (0.08) |
|
Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99) |
6 (0.06) |
|
Diseases of the musculoskeletal system and connective tissue (M00-M99) |
5 (0.05) |
|
Congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) |
5 (0.05) |
|
Diseases of the skin and subcutaneous tissue (L00-L99) |
4 (0.04) |
|
Diseases of the genitourinary sytem (N00-N99) |
3 (0.03) |
|
Diseases of the eye and adnexa (H00-H59) |
3 (0.03) |
|
Neoplasms (C00-D48) |
3 (0.03) |
|
Diseases of the ear and mastoid process (H60-H95) |
2 (0.02) |
|
Pregnancy, childbirth and puerperium (O00-O99) |
1 (0.001) |
41 admissions had more than one diagnosis of personality disorder, meaning that 41 admissions diagnosed with a personality disorder had a comorbid diagnosis of another personality disorder.
Given the fact that 90.7% of comorbid diagnosis belonged to the category of Mental and behavioral disorders (F00-F99), we analyzed this category of comorbid diagnosis separately. The most frequent subcategory within this group of diagnosis belonged to the subcategory F10-F19, followed by the F40-F49 subcategory and the subcategory F30-F39 (Figure 2).
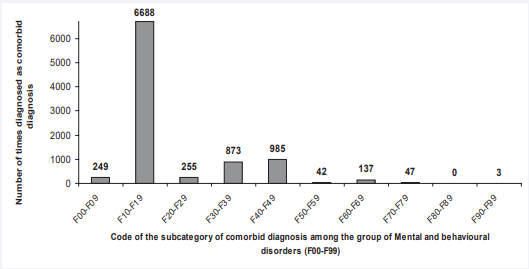
Figure 2: Distribution of comorbidity among the F00-F99 group of comorbid diagnoses between 2000 and 2009.
The F10-F19 subgroup represented 65.7% of all comorbid diagnosis (6,688 out of 10,184) with the most frequent single diagnosis being Alcohol dependence syndrome (F10.2) representing 29.7% of all comorbid diagnosis (3,027 out of 10,184), followed by Acute intoxication with alcohol (F10.0) representing 17.2% of all comorbid diagnosis (1,753 out of 10,184).
The single most frequent diagnosis within the F40-F49 subcategory was Posttraumatic stress disorder (F43.1) representing 3.2% of all comorbid diagnosis (330 out of 10,184). Among the F30-F39 subgroup the most frequent diagnosis was Recurrent depressive disorder, severe episode without psychotic symptoms (F33.2) representing 4.1% of all comorbid diagnosis (422 out of 10,184).
DISCUSSION
We found that the total number of admissions continually increased during the investigated period. Meier [28] conducted a study in two psychiatric hospitals in Burghölzli and Rheinau, Switzerland for the period from 1870 until 1970. Their results also showed a continual increase in admissions during the twenties and thirties (Table 9).
Table 9: Total number of admissions between 1920 and 1939 in two Psychiatric Hospitals in Switzerland compared to Vrap?e Psychiatric Hospital in the same period.
|
|
Number of total admissions between 1920 and 1929 |
Number of total admissions between 1930 and 1939 |
|
Meier, 2009, BurghölzliPsychiatric Hospital, Switzerland |
5970 |
7130 |
|
Meier, 2009, Rheinau Psychiatric Hospital, Switzerland |
12175 |
13280 |
|
Paštaret al, 2010, Vrap?e Psychiatric Hospital, Croatia |
7514 |
8355 |
Rheinau Psychiatric Hospital in Switzerland was designed as a long-term care facility [28] similar to Vrap?e Psychiatric Hospital in Croatia at that time, although at the time Rheinau Hospital had a larger capacity, intended for 600 patients were as Vrap?eHospital had a capacity for 200 – 250 patients [19]. Today Vrap?e Psychiatric Hospital is a contemporary hospital intended to provide acute care as well as care for chronic patients.
Our results showed a more than tenfold increase in the total number of admissions between the thirties and the period from 2000 until 2009, we could not find similar results in literature. Our results for the percentage of admissions discharged with a diagnosis of personality disorder, during the twenties (1.79%) and thirties (2.36%), were considerably lower than results obtained by Meier [28] who found that patients categorized under the diagnostic group ‘’moral qualifications’’ (such as moral insanity or homosexuality) presented 15% of admitted patients for the period from 1916 until 1955. Differences can be explained by the fact that Meier investigated a longer time period as well as the fact that the diagnostic group called ‘’moral qualifications’’ included disorders that do not belong to the category of personality disorders according to the current classifications (MKB i DSM).
We found that 9.97% of all admitted patients between 2000 and 2009 were given the diagnosis personality disorder. Torgersen [29] found that point prevalence of personality disorders is 10%. We cannot state for sure that our results are in concordance with those of Torgensen because we only analyzed the number of admissions with the received diagnosis of personality disorder and our methodology does not reveal whether those admitted patient actually have personality disorders. Furthermore, in our study we included readmissions for the same patient which considerably contributed to the obtained result of 9.97% which was the percentage of admissions with a discharge diagnosis of personality disorder. The contribution of readmissions is even more significant when considering that one patient during the period between 2000 and 2009 was admitted and then discharged 95 times with the diagnosis of personality disorder. We think that the high number of readmissions was a very important finding, opening questions about the connection between personality disorders and readmissions. These questions were partially answered by other investigators who found that a higher risk of readmission is associated to personality disorders [30,31]. In our study we did not further investigate the high number of readmissions even though these findings shed light on all the other results in our study. This is one of the reasons readmissions should be investigated in future studies. Another question that arose from these results was whether a high number of readmissions is related to the psychopathological characteristics of the patient, comorbidity or with the organization of psychiatric care in general. When considering organization of psychiatric care, it is important to emphasize that our data showed that 53.8% of admitted patients during the period between 2000 and 2009 were unemployed and 21.2% were retired. As we could not find any research done receiving similar results to these in Croatia, we were unable to comment possible differences. We can, however, emphasize the questions arising from these finding: Are personality disorders disabling disorders and as such causing the majority of our admitted patients to be unemployed? What is the nature of such a disability? Can such disabilities be observed through the prism of mental illness and its consequences? Is the high rate of unemployment a conscious decision made by persons with personality disorders living in today’s day? These questions have an even greater value when considering the results obtained from the twenties and thirties when unemployment was only 14.2% and 9.6%, respectively. Furthermore, these results pose questions about the cost of hospitalisation and its burden on the health care system and on society. This burden is even “heavier” as we are unsure whether to consider personality disorders as an illness, disorder, conscious or unconscious manipulation. Furthermore our results showed that the percentage of admitted patients sent to hospital by courts or police decreased from 62.9% in the twenties, to 15.7% in the thirties and then to 1.3% in the period from 2000 until 2009, can this be connected to the above mentioned “manipulation,” of patients with personality disorders, who are becoming aware that they can go through life unemployed and “protected” in hospital? Or does such data indicate that there is a greater general awareness of the difficulties that arise from personality disorders? We could not find similar data in literature, so these questions are still to be answered.
Our results showed that 22.7% of admitted patients with the diagnosis of personality disorder were divorced, we could not find similar data in Croatia, but studies done by South et al andWhisman and Schonbrun [32,33] showed similarly that having a personality disorder significantly contributed to marital disrupt.
We found that the average length of stay in hospital significantly decreased during the investigated periods (during the twenties: 92 days, during the thirties: 80 days, from 2000 until 2009: 10 days). Does this finding mean that the treatment of personality disorders is becoming more efficient over time? If this is true, why is the number of readmissions considerably higher than in the earlier decades (95 readmissions during the period from 2000 until 2009)? Is there a connection between the shorter length of stay in hospital and the higher number of readmission? We could not find published data on this topic, so these questions are also to be answered in future studies.
When considering the nomenclature of personality disorders during the twenties and thirties, our results showed 10 (during twenties) and 20 (during thirties) different types of personality disorders, which at first glance differs from the findings of Partridge [25,26]. He delineated three types of Psychopathy in his study: Delinquent type, inadequate type and general incompatibility type but he concluded that “psychopath is one whom strong demands are accompanied by feelings of inadequacy, inferiority or insecurity and in whom there develops a tendency to resort to one or more typical reaction patterns, different in different cases, but all to be included in a general way under tantrums, sulks and running away” [34]. Upon closer evaluation our results are similar to those of Partridge if considering the fact that the majority of our admitted patients were termed as psychopathy which can be connected to Partridge’s conclusion that all can ‘’be included in a general way under tantrums, sulks and running away”. Along with psychopathy we found additional terms used, like psychopathiashizoides, paranoides, with hysterical traits etc. These additional terms can also fit into Partridge’s conclusion of a “tendency to resort to one or more typical reaction patterns, different in different cases.”
In Croatia no systematic studies on the prevalence of personality disorders among inpatients have been published. Our results showed a 26.6% prevalence of the diagnosis of emotionally unstable personality disorder and a 24.2% prevalence of the diagnosis of dissocial personality disorder which is in concordance to data from DSM-IV [2] where it is stated that the prevalence of Emotionally unstable personality disorder is between 30% and 60% among inpatients having personality disorders and the prevalence of Dissocial personality disorder is between 3% and 30% among psychiatric inpatients. For other types of personality disorders our results differed from those in DSM-IV [2].
In terms of comorbidity, we found an extreme difference in the percentage of admitted patients with comorbidity during the investigated period. During the twenties and thirties that percentage was no higher than 23.7%, and then during the period between 2000 and 2009 it increased to 90.4%. Similar comparisons could not be found in literature. This very significant difference can be explained by the fact that diagnostics are more advanced today than they were in the twenties and thirties, we are also more aware of the importance of noting all comorbidity not only for medical but also legal reasons [35]. For the periods from 1930 – 1939 and 2000 – 2009 we found that the most frequent single comorbid diagnosis was Alcoholism (in recent decade coded as F10.2). We are quite certain that the high number of readmissions during the recent decade is connected to Alcoholism being the most frequent comorbid diagnosis, although we did not prove this in our study. What is the true connection between personality disorders and comorbidity? Is the increase in comorbidity misleading us into giving diagnosis of personality disorder to those persons who actually are not suffering from personality disorder? Or is the other way around, the increase in personality disorders being responsible for the high percentage of comorbidity? These questions are still to be answered in future studies.
REFERENCES
- World Health Organisation. ICD-10, chapter V (F). Zagreb: Medicinskanaklada; 1994.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Fourth Edition (DSM IV). Washington (DC): APA; 1994.
- Loranger AW, Janca A, Sartorius N. Assessment and diagnosis of personality disorders. The ICD-10 international personality disorder examination (IPDE). New York: Cambridge University Press; 2007.
- Korzekwa M, Links P, Steiner M. Biological markers in borderline personality disorder: new perspectives. Can J Psychiatry. 1993; 38: 11-15.
- Lahmeyer HW, Reynolds CF 3rd, Kupfer DJ, King R. Biologic markers in borderline personality disorder: a review. J Clin Psychiatry. 1989; 50: 217-225.
- Gelernter J, Kranzler H, Coccaro E, Siever L, New A, Mulgrew CL. D4 dopamine-receptor (DRD4) alleles and novelty seeking in substance-dependent, personality-disorder, and control subjects. Am J Hum Genet. 1997; 61: 1144-1152.
- Ni X, Chan K, Bulgin N, Sicard T, Bismil R, McMain S, et al. Association between serotonin transporter gene and borderline personality disorder. J Psychiatr Res. 2006; 40: 448-453.
- Stalenheim EG. Long-term validity of biological markers of psychopathy and criminal recidivism: follow-up 6-8 years after forensic psychiatric investigation. Psychiatry Res. 2004; 121: 281-291.
- Tadi? A, Baskaya O, Victor A, Lieb K, Höppner W, Dahmen N. Association analysis of SCN9A gene variants with borderline personality disorder. J Psychiatr Res. 2008; 43: 155-163.
- Martins IJ. Diabetes and Organ Dysfunktion in the Developing and Developed. Worl Journal of Medical Research: F Diseases. 2015.
- Martins IJ. The Global Obesity Epidemic is Related to Stroke, Dementia and Alzheimer’s disease. JSM Alzheimer’s Dis Related Dementia. 2014; 1: 1010.
- Martins IJ. Magnesium Therapy Prevents Senescence with the Reversal of Diabetes and Alzheimer’s Disease. Health. 2016; 8: 694-710.
- Martins IJ. Diet and Nutrition reverse Type 3 Diabetes and Accelerated Aging linked to Global chronic diseases. J Diab Res Ther. 2016; 2.
- Martins IJ. Type 3 diabetes with links to NAFLD and Other Chronic Diseases in the Western World. Int J Diabetes. 2016; 1:1-5.
- Martins IJ. Induction of NAFLD with Increased Risk of Obesity and Chronic Diseases in Developed Countries. OJEMD. 2014: 4: 90-110.
- Martins IJ. Unhealthy Nutrigenomic Diets Accelerate NAFLD and Adiposity in Global communities. J Mol Genet Med. 2015; 9.
- Mela M, Audu M, Tesfaye M, Gurmu S. A developing world perspective on homicide and personality disorder. Med Sci Law. 2014; 54: 132-138.
- Tyrer P, Mulder R, Crawford M, Newton-Howes G, Simonsen E, Ndetei D, et al. Personality disorder: a new global perspective. World Psychiatry. 2010; 9: 56-60.
- Pastar Z, Petrov B, Krizaj A, Bagaric A, Jukic V. Diagnoses of personality disorders between 1879 and 1929 in the largest Croatian psychiatric hospital. Croat Med J. 2010; 51: 461-467.
- Wittchen HU. Critical issues in the evaluation of comorbidity of psychiatric disorders. Br J Psychiatry Suppl. 1996; 9-16.
- Feinstein AR. The Pre-Therapeutic Classification of Co-Morbidity in Chronic Disease. J Chronic Dis. 1970; 23: 455-468.
- Burke JD, Wittchen HU, Regier DA, Sartorius N. Extracting information from diagnostic interviews on cooccurrence of symptoms of anxiety and depression. In: Maser JD, Cloninger CR, editors. Comorbidity of Mood and Anxiety Disorders. Washington (DC): APP; 1990: 649-667.
- Prichard JC. Moral Insanity. Hist Psychiatry. 1999; 10: 117-126.
- Berrios GE. J.C. Prichard and the concept of "moral insanity". Classic text no.37. Hist Psychiatry. 1999; 10: 111-126.
- Berrios GE. European views on personality disorders: a conceptual history. Compr Psychiatry. 1993; 34: 14-30.
- Koch JLA. The psychopathic inferiorities. Ravensburg (Germany): Dorn; 1891.
- Schneider K. Psychopathic personalities. London: Cassell; 1950.
- Meier M. Creating order.A quantitative analysis of psychiatric practice at the Swiss mental institutions of Burghölzli and Rheinau between 1870 and 1970. Hist Psychiatry. 2009; 20: 139-162.
- Torgersen S. The nature (and nurture) of personality disorders. Scand J Psychol. 2009; 50: 624-632.
- Prince JD, Akincigil A, Kalay E, Walkup JT, Hoover DR, Lucas J, et al. Psychiatric rehospitalization among elderly persons in the United States. Psychiatr Serv. 2008; 59: 1038-1045.
- Korkeila JA, Lehtinen V, Tuori T, Helenius H. Frequently hospitalised psychiatric patients: a study of predictive factors. Soc Psychiatry Psychiatr Epidemiol. 1998; 33: 528-534.
- South SC, Turkheimer E, Oltmanns TF. Personality disorder symptoms and marital functioning. J Consult Clin Psychol. 2008; 76: 769-780.
- Whisman MA, Schonbrun YC. Social consequences of borderline personality disorder symptoms in population-based survey: marital distress, marital violence and marital disruption. J Pers Disord. 2009; 23: 410-415.
- Partridge GE. A study of 50 cases of psychopathic personality. Am J Psychiatry. 1927; 7: 953-974.
- Partridge GE. Current conceptions of psychopathic personality. Am J Psychiatry. 1930; 10: 53-99.








































































































































