Rare Localizations of Metastatic Osteosarcoma: A Case Report of Subcutaneous and Cervical Lymph Node Involvement
- 1. Department of Pulmonology, 20 August 1953 Hospital, Morocco
Abstract
Malignant transformation of osteosarcoma is a rare but severe complication that can occur in patients who have previously been treated for low-grade osteosarcoma. This complication is particularly concerning as it can lead to rapid deterioration of the patient’s condition and a significant decrease in their chances of survival. The risk factors for this complication are still poorly understood, but it is acknowledged that patients who have received incomplete or insufficient initial treatment are more likely to develop malignant transformation. We report the case of a 20-year-old man who developed malignant transformation of his low-grade osteosarcoma, treated with tumor resection without adjuvant therapy. The patient presented 2 years after conservative surgery with pulmonary metastases, as well as rare subcutaneous and cervical lymph node metastases. These latter metastases are particularly unusual and represent an additional challenge in patient management. This clinical case highlights the importance of multidisciplinary care in improving outcomes for patients with osteosarcoma. Regular surveillance and comprehensive evaluation of patients are essential for early detection of metastases and adapting management. The complexity of this rare condition requires an individualized approach, taking into account the specific characteristics of each patient. Further research is necessary to improve outcomes for patients with osteosarcoma.
Citation
Nahidi M, Bougteb N, El Khattabi W, Arfaoui H, Msika S, et al. (2026) Rare Localizations of Metastatic Osteosarcoma: A Case Report of Subcutaneous and Cervical Lymph Node Involvement. Ann Orthop Rheumatol 12(1): 1104.
INTRODUCTION
Osteosarcoma is an aggressive bone cancer that primarily affects children and adolescents. It is the most common type of bone cancer in young people, and is characterized by rapid and invasive growth of cancer cells in the bones. Despite advances in the treatment of this disease, metastases remain a major complication that affects patient survival and quality of life. Metastases are the spread of cancer cells from the initial tumor site to other parts of the body. In the case of osteosarcoma, metastases can form in various organs, such as the lungs, bones, brain, and lymph nodes. Among the different metastatic sites, cervical lymph node metastases are particularly rare and represent a diagnostic and therapeutic challenge. We present here the case of a 20-year-old patient who has been followed for a low-grade osteosarcoma for 2 years. Despite initial effective treatment, the patient developed a cervical lymph node and subcutaneous metastases, which represent a challenge for the management of his disease. This case illustrates the diagnostic and therapeutic challenges associated with this rare complication and highlights the importance of multidisciplinary management to improve outcomes for these patients.
CASE REPORT
The patient is a 20-year-old student with no toxic habits. He presented 2 years ago with a low-grade osteosarcoma, characterized by a painful swelling of the right knee and a deterioration of his general condition. Following his diagnosis, conservative surgery was indicated, and the postoperative course was uncomplicated. He did not receive adjuvant chemotherapy or other therapeutic interventions. The 2-year follow-up was marked by a local recurrence of his osteosarcoma, manifesting as a new mass at the knee level. Histopathological examination of the new knee mass revealed a malignant transformation of the low-grade osteosarcoma, characterized by increased cellular atypia and mitotic activity. He also presented with progressive dyspnea and a dry cough, which had evolved over 5 months. His general condition was altered, with a performance status (PS) of 2. On physical examination, he was eupneic, with oxygen saturation at 95% on room air. He had a tachycardia of 105 beats per minute. The rest of his vital signs were within normal limits. Respiratory examination revealed a left-sided pleural effusion syndrome. He also presented with a painful swelling of the right lower limb (Figure 1),
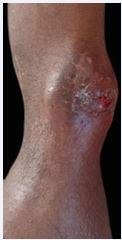
Figure 1 Mass on the right lower limb.
multiple subcutaneous nodules on his back (Figure 2), and three lower cervical lymphadenopathies, with the rest of the clinical examination being normal. Chest radiography performed on admission showed multiple bilateral rounded opacities with a left-sided pleural opacity (Figure 3). Thoracic ultrasound revealed a multi-septated left-sided pleural effusion. Thoracic CT scan showed a left lower lobe pulmonary process with bilateral cannonball lesions, a minimal left sided pleural effusion, and mediastinal lymphadenopathies (Figure 4).

Figure 2 Subcutaneous back nodules.

Figure 3 Chest X-ray (AP view).

Figure 4 Thoracic CT scan.
At this stage, the diagnosis of metastatic osteosarcoma was the most likely, given the presence of multiple pulmonary nodules with a history of osteosarcoma. However, the presence of subcutaneous nodules and cervical lymphadenopathies was atypical for metastatic osteosarcoma, and the possibility of a second primary malignancy, such as bronchogenic carcinoma, was considered. Flexible bronchoscopy revealed a tumor-like infiltration of the left lower lobe. Histopathological examination it biopsy showed a malignant fusiform and aggressive tumor proliferation consistent with osteosarcoma. (Figure 5).

Figure 5 Histology.
Cervical ultrasound confirmed the presence of 3 lower cervical lymphadenopathies with calcifications, which prompted a cervical lymphadenectomy. Histopathological examination of the lymphadenectomy was consistent with a secondary localization of osteosarcoma.
Biopsy of one of the subcutaneous nodules on the back also showed a histopathological examination consistent with a secondary localization of his knee osteosarcoma.
This case represents a rare instance of malignant transformation of a low-grade osteosarcoma in a young adult, with multiple metastases involving the lungs, subcutaneous tissue, and cervical lymph nodes. Notably, the presentation of subcutaneous and cervical lymph node metastases is extremely rare in osteosarcoma and this unusual presentation makes this case report particularly pertinent, as it highlights the importance of considering osteosarcoma in the differential diagnosis of patients presenting with subcutaneous nodules and cervical lymphadenopathies. It also underscores the need for a multidisciplinary approach to managing complex cases of metastatic disease.
The multidisciplinary thoracic oncology meeting recommended initiating chemotherapy with a combination of methotrexate, adriamycin, and cisplatin. This treatment plan was chosen based on the patient’s age, the extent of his disease, and the histopathological characteristics of his tumor.
The patient’s prognosis is guarded, given the aggressive nature of his disease and the presence of multiple metastases. However, with prompt and aggressive treatment, there is hope for improving his symptoms and prolonging his survival.
DISCUSSION
Osteosarcoma is a malignant tumor that develops in the bones. It is the most common form of primary bone cancer, accounting for approximately 5% of all cancers in children and adolescents [1]. Osteosarcoma is characterized by the production of bone matrix by tumor cells, leading to the destruction of normal bone and the formation of new, abnormal bone structures [2]. Osteosarcoma can develop in any part of the bone, but it is more common in long bones, such as the femur, tibia, and fibula [3]. Symptoms of osteosarcoma may include bone pain, swelling, limited mobility, and pathological fractures [4].
There are different types of osteosarcomas, including high-grade and low-grade osteosarcoma. Low grade osteosarcoma is a malignant tumor with lower aggressiveness compared to high-grade osteosarcoma. Low-grade tumours are generally characterized by slow growth, conserved cellular differentiation, and low aggressiveness. The transformation to high-grade osteosarcoma is often associated with genetic and epigenetic alterations that affect cell growth regulation and differentiation. The factors that contribute to this transformation are not yet fully understood, but it is thought that factors such as genetic mutations, epigenetic changes, and interactions between tumor cells and their environment play an important role.
Osteosarcoma is a rare disease, with an annual incidence of approximately 3-4 cases per 1 million inhabitants [5]. It is more common in adolescents and young adults, with a peak incidence between 15 and 19 years [6]. Boys are more often affected than girls, with a ratio of 1.5 to 2 to 1 [7]. The incidence of osteosarcoma varies depending on geographic region and population studied [8]. In developed countries, the incidence of osteosarcoma is higher than in developing countries [9].
Several risk factors have been identified for osteosarcoma, including:
- Age: osteosarcoma is more common in adolescents and young adults.
- Sex: men are more often affected than womens
- Height: people of tall stature are at increased risk of developing osteosarcoma.
- Family history: individuals with a family history of bone cancer or genetic syndromes such as Li-Fraumeni syndrome are at increased risk of developing osteosarcoma.
- Environmental exposures: people exposed to chemicals such as pesticides or industrial chemicals may be at increased risk of developing osteosarcoma.
- Ionizing radiation: people exposed to ionizing
radiation, such as X-rays or gamma rays, may be at increased risk of developing osteosarcoma.
The diagnosis of osteosarcoma is based on a combination of clinical examinations, imaging tests, and biopsies [1]. Clinical examinations include medical history, physical examination, and tests of bone and joint function [2]. Imaging tests include X-rays, computed tomography (CT) scans, magnetic resonance imaging (MRI) scans, and bone scans [3]. Biopsies are tissue samples that are examined under a microscope to detect the presence of cancer cells.
The stages of osteosarcoma are as follows:
- Stage I: the tumor is localized and has not invaded the surrounding tissues.
- Stage II: the tumor has invaded the surrounding tissues, but has not reached the lymph nodes.
- Stage III: the tumor has reached the lymph nodes.
- Stage IV: the tumor has reached distant metastases.
There are other classifications of osteosarcoma, such as the American Joint Committee on Cancer (AJCC) classification and the International Federation of Orthopaedic Surgery and Traumatology (SICOT) classification.
In our case, the patient has a tumor of 8 cm in diameter, with cervical lymph node metastases and subcutaneous metastases. Therefore, the patient is classified as having stage IV osteosarcoma, according to the TNM classification system.
The treatment of osteosarcoma depends on several factors, such as the stage of the disease, the location of the tumor, and the presence of metastases. In the case of our patient, who presents with a malignant transformation of a low-grade osteosarcoma with multiple pulmonary, cervical lymph node, and subcutaneous metastases, treatment will need to be tailored to take into account these factors.
Chemotherapy is an essential treatment for osteosarcoma, particularly for patients with metastases [2]. Osteosarcoma chemotherapy protocols typically include a combination of drugs such as doxorubicin an anthracycline antibiotic that interferes with the growth of cancer cells, cisplatin, platinum-based drug that damages the DNA of cancer cells and methotrexate an antimetabolite that interferes with the growth of cancer cells [1]. In the case of our patient, chemotherapy will likely be used to treat the pulmonary, cervical lymph node, and subcutaneous metastases.
Surgery and radiation therapy are also an important treatment for osteosarcoma, particularly for patients with localized tumors. However, in the case of our patient, who presents with multiple metastases, they are not indicated.
For our patient who presented with a malignant transformation of a low-grade osteosarcoma with multiple pulmonary, cervical lymph node, and subcutaneous metastases, it is essential to implement a rigorous follow- up and surveillance plan to detect any recurrence or progression of the disease.
- The follow-up plan for our patient should include:
- Regular physical exams to monitor for signs of recurrence;
- X-rays and CT scans to monitor the size of the tumor and metastases;
- Blood tests to monitor kidney and liver function;
- Regular consultations with the medical team to discuss test results and potential modifications to the treatment plan.
Research on osteosarcoma is constantly evolving, and new therapeutic approaches are being explored. Here are some of the most promising ones:
- Targeted Therapy: Protein kinase inhibitors, such as pembrolizumab and nivolumab, have shown promising results in treating osteosarcoma [1].
- Stem Cell Therapy: stem cell therapy involves using stem cells to repair or replace damaged tissues. Research is ongoing to explore the use of this therapy in treating osteosarcoma [10].
- Immunotherapy: immunotherapy involves stimulating the immune system to attack cancer cells. Research is ongoing to explore the use of this therapy in treating osteosarcoma [1].
- Nanoparticle Therapy: nanoparticles can be used to target cancer cells and deliver drugs in a specific manner [11].
- RNA Interference Therapy: RNA interference can be used to inhibit the expression of specific genes involved in the progression of osteosarcoma [1].
Research has shown that genetic and epigenetic alterations play a crucial role in the development of osteosarcoma. Here are some of the most common alterations [1]:
- TP53 Gene Mutations: the TP53 gene is a tumor suppressor gene that plays a critical role in regulating cell growth. Mutations in this gene are common in osteosarcoma.
- RB1 Gene Mutations: the RB1 gene is a tumor suppressor gene that plays a critical role in regulating cell growth. Mutations in this gene are common in osteosarcoma.
- Gene Expression Alterations: gene expression alterations can be caused by epigenetic modifications, such as DNA methylation or histone acetylation. These alterations can lead to the overexpression or underexpression of genes involved in osteosarcoma progression.
The prognosis of osteosarcoma depends on several factors, including the location of the tumor, the size of the tumor, the patient’s age, the presence of metastases, and the response to treatment. Many scores have been developed for osteosarcoma, such as:
- The San-Julian score: This score takes into account the patient’s age, the location of the tumor, and the presence of metastases to predict the patient’s prognosis. The score of our patient is 4.
- The MSTS (Musculoskeletal Tumor Society) score: This score takes into account the functionality of the affected limb, pain, and mobility to predict the patient’s prognosis. The score of our patient is 3.
These scores indicate a reserved prognosis for your patient. The presence of metastases and the size of the tumor are unfavorable factors.
It is essential to note that these scores are not always accurate and should be used in combination with other factors to predict the patient’s prognosis.
CONCLUSION
Osteosarcoma is a type of bone cancer that requires early diagnosis and multidisciplinary treatment to improve outcomes for patients. The diagnosis of osteosarcoma is based on a combination of clinical examinations, imaging tests, and biopsies. The case of our patient, is particularly interesting. He presents with a malignant transformation of his low-grade osteosarcoma with rare localizations of metastases. This clinical case highlights the complexity and variability of osteosarcoma. It emphasizes the importance of taking into account the specific characteristics of each patient to determine the best treatment approach and it illustrates the importance of multidisciplinary care and the need to continue research to improve outcomes for patients with osteosarcoma.
We finally recommend that patients with osteosarcoma be followed up regularly so the recurrences and metastases be detected early to improve outcomes. It is also essential to continue research to develop new therapies and improve understanding of this disease.
REFERENCES
- National Cancer Institute. Osteosarcoma Treatment (PDQ) - Health Professional Version. 2020.
- American Cancer Society. Osteosarcoma. 2020.
- Mayo Clinic. Osteosarcoma. 2020
- Damron. Malignant transformation of low-grade osteosarcoma. J Bone and Joint Surg. 2007; 89: 1131-1136.
- Whelan. Treatment of osteosarcoma. J Clin Oncol. 2018; 36: 2244-2251.
- Ferrari. Chemotherapy for osteosarcoma. J Pediatric Hematology/ Oncology. 2018; 40: 351-355.
- Anninga. Metastatic patterns in osteosarcoma. J Bone and Joint Surg. 2011; 93: 1054-1060.
- Edge. AJCC Cancer Staging Manual. New York: Springer.2010.
- Radiation Oncology. Osteosarcoma: Radiation Therapy. 2018.
- Journal of Clinical Oncology. Stem Cell Therapy for Osteosarcoma. 2019.
- Nature Nanotechnology. Nanoparticle-based therapy for osteosarcoma. 2020.









































































































































{kind=link}