Electronic Media Use at Bedtime in Early Childhood
- 1. Department of Sleep Medicine, San Antonio Military Health System, USA
- 2. Department of Sleep Medicine, University of Maryland School of Medicine, USA
ABSTRACT
Nighttime use of electronic media (EM) including smartphones and tablets is reported to have detrimental effects on sleep. Survey-based studies demonstrate that EM use near bedtime and in bed is associated with shortened sleep duration and insomnia in adults and children. This report describes the case of a 3-year old boy who repeatedly used a smartphone while undergoing an attended in-lab polysomnogram (PSG). The child’s PSG results provide objective evidence supporting the adverse effects of EM on sleep quality and suggest a potential pathway for development of chronic insomnia. Providers should ask about EM use in young children with complaints of insomnia or restless sleep.
KEYWORDS
• Electronic
• Pediatric
• Sleep
• Insomnia
CITATION
Foster SN, Mysliwiec V, Wickwire E, Brock MS (2016) Electronic Media Use at Bedtime in Early Childhood. Ann Pediatr Child Health 4(3): 1109.
ABBREVIATIONS
EM: Electronic Media; PSG: Polysomnogram; OSA: Obstructive Sleep Apnea; AHI: Apnea-Hypopnea Index.
INTRODUCTION
Electronic media are widely used in all age groups. Although these technologies are integral to multiple aspects of modern living, survey-based studies consistently report high prevalence of nighttime EM use and resultant adverse effects on sleep. Up to 54% of school-aged children admit to sleeping near a small screen, such as a smartphone or tablet [1]. Further, children who sleep near a screen or use EM prior to falling asleep have delayed sleep onset, shorter sleep duration, and perceive their sleep as insufficient [1,2]. Similar findings were reported in adults, with EM use in bed associated with both insomnia and shorter sleep duration [3]. There is evidence that the adverse effects of EM use on sleep may be persistent. In adolescents, texting and/or phone use after lights out was associated with feeling very tired 1 year later [4]. The adverse effects of EM use at bedtime may also impact very young children (i.e. preschool), though a paucity of data exists in this age group. This case report describes a 3-year old boy who used a smartphone during an in-lab PSG. His PSG provides objective evidence for the potential of EM use in bed to result in markedly disturbed sleep in young children.
CASE PRESENTATION
A 3 year old boy was referred to an AASM-accredited sleep disorders center for evaluation of a one-year history of irregular sleep schedule, frequent nighttime awakenings, and snoring. Physical airway examination was notable for 2+ tonsils. He also suffered seasonal allergies, which were treated with montelukast, loratadine, and nasal fluticasone. To evaluate for the presence of organic sleep disorders and rule-out obstructive sleep apnea (OSA), the patient underwent an attended in-lab PSG. His PSG demonstrated increased wake after sleep onset of 167.8 minutes, an arousal index of 10.2/hour, and a decreased sleep efficiency of 63.6%. He had a mildly elevated apnea hypopnea index (AHI=1.8). Of particular interest, review of nocturnal video recording revealed the child spending a considerable portion of the sleep period playing with his mother’s smartphone (Figure 1).
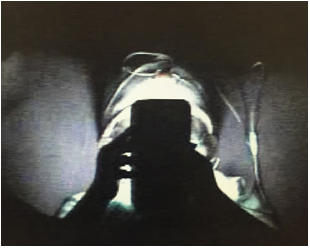
Figure 1: Child using smartphone during overnight sleep study.
This occurred prior to “lights out” and throughout the PSG. During awakenings in the first half of the night, the child’s mother would hand him her smartphone to provide comfort. He continued to use the device as late as 0200, long after his mother had fallen asleep. The sleep technologist did not intervene. During the follow up visit after the PSG, further history revealed regular nightly use of EM at bedtime. The patient was diagnosed with inappropriate sleep practices and mild OSA. The family was counseled on appropriate sleep practices including avoidance of EM near bedtime and in bed. The mother reported significant improvement in her son’s sleep quality almost immediately after restricting his use of EM in the bedroom. They opted for conservative management of his mild OSA with a follow-up PSG in the future.
DISCUSSION
To our knowledge, this is the first report to objectively demonstrate the adverse effects of EM on sleep in a young child referred for evaluation of frequent awakenings and snoring. Although sleep apnea may have partially contributed to his difficulty sleeping, PSG results revealed that most of his awakenings were not due to respiratory events. It is also unclear whether the boy learned to use EM in bed for comfort or from continuation of habitual daytime use. Nonetheless, his primary diagnosis of inappropriate sleep practices due to EM was substantiated by the marked clinical improvement with removal of EM from his bedroom.
A growing body of evidence highlights the detrimental effects of bedtime EM use on sleep. In a crossover study of 12 healthy adults, when compared to reading a physical book, reading an e-reader for approximately 4 hours prior to sleep resulted in increased sleep onset latency and decreased REM sleep but had no impact on total sleep time [5]. In children, it is possible that these effects are magnified. The interactive nature of some EM likely results in increased sleep disturbance relative to a static device such as an e-reader. In our patient, review of video evidence suggests that this interactivity contributed to his difficulty falling and staying asleep. Providers should be cognizant of the effects EM have on sleep and counsel their patients against use of EM near bedtime and in the bedroom.
CONFLICT OF INTEREST
No financial support was provided for this project. Drs. Foster, Mysliwiec, and Brock have no conflicts of interest to disclose. Dr. Wickwire has moderated non-commercial scientific discussion for Merck and is an equity stakeholder in WellTap (R), which provides online patient screening and education.







































































































































{kind=link}