Pericardial Effusion on CXR, an aide-memoir
- 1. Department of Paediatric Cardiology, Royal Belfast Hospital for Sick Children, USA
- 2. Queens University Belfast, University Rd, USA
CITATION
Kendall S, McGinn C, Sands A (2023) Pericardial Effusion on CXR, an aide-memoir. Ann Pediatr Child Health 2023; 11(5): 1324.
INTRODUCTION
Chest pain in children is a common presentation to the Emergency Department (ED). Whilst cardiac causes are uncommon, they are important and should be considered in the context of a suspicious history and clinical examination. The vast majority of chest pain in children is non-cardiac in origin. However the clinician needs to be aware of red flag symptoms, signs and investigation findings.
CASE REPORT
An 11-year-old female presented to a tertiary paediatric ED with a nine-day history of intermittent chest pain, exacerbated by lying flat and associated pyrexia. She had no significant past medical history. She appeared pale, was tachycardic and had soft heart sounds, her blood pressure was normal. A plain chest radiograph (CXR) is demonstrated in Figure 1.
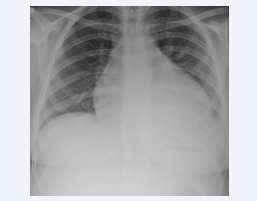
Figure 1: CXR demonstrating globular cardiomegaly, the “water bottle sign,” effacement of the left costo-phrenic angle & air space opacification in the retrocardiac region.
She then underwent an echocardiogram which demonstrated a large global pericardial effusion with mildly reduced biventricular systolic function. She was treated with IV Ceftriaxone, Colchicine, Ibuprofen and Prednisolone. The cause for the effusion was not confirmed but improved following the above treatment.
DISCUSSION
Pericardial effusions are definitively diagnosed with echocardiography and when small can be difficult to appreciate on plain-film radiography. However signs suggestive on CXR include globular enlargement and the so called “water bottle sign” [1], in which the pericardium has been gradually stretched causing it to sag bilaterally mimicking a hot water bottle (Figure 2).

Figure 2: Half-filled hot water bottle.
Other signs on CXR include serially enlarging cardiothoracic ratio, pulmonary oedema, pleural effusion and in some cases widening of the sub-carinal angle [2].









































































































































{kind=link}