A New Type of Occipital Condyle Fractures - A Case Report and Revision of Literature is Presented
- 1. Department of Orthopedics and Spine Surgery, Hospital Regional de São José Dr Homero de Miranda Gomes, Brazil
Abstract
The authors report a very rare case of bilateral occipital condyle fractures (OCF) that was associated with complete separation fracture of the inferior clivus resulting in craniocervical dislocation alongside dissociation of C1-C2 joint complex. Also, a new type of the Anderson and Montesano’s classification system is presented with two subtypes of injuries. Type IVA occurs when the OCF is associated a clivus avulsion fracture whilst Type IVB occurs when the OCF is associated with complete ‘en piece’ separation fracture of the inferior clivus. Both Type IV injuries are considered highly unstable and surgical fixation is the recommended treatment option.
Keywords
Occipital condyle fracture, Clivus fracture, Occipitocervical dislocation, Craniocervical injury, Anderson and Montesano
Citation
Carriço G, Lam KS (2022) A New Type of Occipital Condyle Fractures - A Case Report and Revision of Literature is Presented. Ann Sports Med Res 9(1): 1186.
INTRODUCTION
Occipital condyle fractures (OCF) was first described by Bell [1] in 1817 and continues to be a diagnostic challenge to all spine surgeons. OCF are rare injuries that are made more challenging because they are not easily visible on conventional craniocervical spine X-rays.
The most common classification system used in OCF was described by Anderson and Montesano [2] in 1988. In 1997, Tuli et al. [3], suggested a new classification system that also divided the fractures into 3 different types with the inclusion of the craniocervical junction (Table 1). High index of suspicion of this kind on injury helps to guide the spine surgeon towards successful management of these potentially devastating injuries [4].
Herein the authors report a very rare case of bilateral OCF associated with complete ‘en piece’ separation fracture of the inferior clivus alongside dissociation of C1-C2 joint complex. According to the published English literature, this fracture configuration has never been described before nor can it be classified using the conventional classifications systems. Authors reviewd the English literature on OCF that are associated with fractures of the clivus and hereby present a new type of Anderson and Montesano’s fracture that could be included as OCF fourth type.
CASE PRESENTATION

Figure 1: Axial CT section show bilateral occipital condyle fractures (yellow dotted arrows).
We report a 21-year-old male who was involved in a high energy motor vehicle accident (MVA) and was subsequently ejected 20 meters out from his car. His immediate Glasgow coma scale (GCS) was 6 and he was intubated at the scene. Physical examination at that time revealed a large hematoma on the right side of his skull and a globally dense right-sided hemiparesis (2- 3/5 power on the medical research council [MRC]).
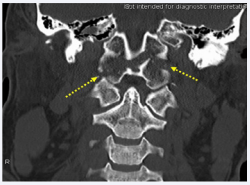
Figure 2: Coronal CT shows bilateral occipital condyle fractures (yellow dotted arrows).
CT images revealed bilateral OCF (Figure 1 and 2) extending into the inferior part of the clivus (Figure 3), fracture of the lateral masses of C1, widening of the atlantooccipital joint space and disruption of the C1-C2 posterior interspinous distance causing severe craniocervical dislocation with gross instability.

Figure 3: Lateral CT shows ‘en piece’ fracture of the clivus (yellow dotted arrow).
A halo-vest was applied same day of injury and posterior occipito-C1-C2 fixation using C1 lateral mass and C2 pedicle screws was performed five days later (Figure 4). Patient was extubated four days after surgery, moving his four limbs with slight deficit on his right side.

Figure 4: Lateral post op radiographs of the cervical spine
t sixty days after surgery he became increasingly ataxic and his brain MRI showed an area of acute epidural fibrosis at C0-C1 subsequent to the resolving subarachnoid hematoma resulting in acute hydrocephalus. This necessitated an urgent posterior fossa decompression via a C1 laminectomy followed by insertion of a ventricular peritoneal shunt some nine days later.
At one year following the accident, patient was pain-free with minimal right leg weakness. Brain and cervical spine MRIs showed no evidence of persistent hydrocephalus and CT of the craniocervical junction showed complete fracture union. At two years, he represented with occasional headaches alongside a stiff but painless neck. Further repeat MRI showed persistent myelomalacia changes at C2 but he was neurologically normal. Patient has regained full neurological recovery and is now leading a normal life.
DISCUSSION
We have identified only 6 descriptions in the English literature reporting the association of bilateral OCF associated with an avulsion fracture of the inferior clivus. OCF are rare and therefore almost all available data are retrospective and sometimes based on a small series of cases [5-7]. The initial reports came from autopsy series [8,9] and case reports. CT is considered the gold standard investigation of choice when diagnosing OCF [10,11].
The main cause of OCF is high energy MVA trauma that is associated severe traumatic brain injury [10,12,13] caused by blunt head trauma. In a large autopsy series of victims with head trauma, the incidence of OCF ranged from 0.6 to 4.2% [8,14].
The most common clinical feature in the trauma setting is loss of consciousness [15-20]. Also, cranial nerve damage can occur, mainly the XII pair, but also the IX, X and XI cranial nerves can be involved. In some cases, unilateral palsy of the last four cranial nerves may occur, a.k.a., the Collet-Sicard syndrome [5].
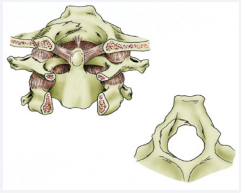
Figure 5: Type IV A: OCF + clivus avulsion fracture
Reza et al.[4], believed that the mechanism of injury is axial loading and compression. We hypothesize that axial loading and compression occured in our case, similar to the ‘nut-cracker’ effect.
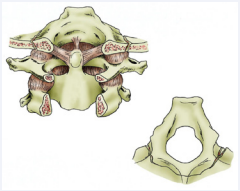
Figure 6: Type IV B: OCF + complete ‘in piece’ fracture separation of the clivus.
Both Anderson and Montesano [2] and Tuli et al. [3], classification systems do not describe this fracture subtype as seen in our case. We propose a novel type IV injury (OCF associated with clivus fracture), and furthermore subdivide this into type IVA [OCF associated with an avulsion fracture of the clivus (Figure 5)] and type IVB [OCF associated with ‘en piece’ fracture of the clivus (Figure 6)] (Table 1). Both sub-types are considered unstable and the type IVB is a highly unstable injury and therefore both sub-types require surgical stabilisation. Understandably although we appreciate that only one case report may not enough to modify a classification system, but when dealing with this extremely rare type of fracture that has been only reported six times before our case, we believe that adding these injuries offers a useful guide when managing OCF.
| Type | Description | Stability |
|---|---|---|
|
I
|
Impacted fracture Fracture of the base of the skull extending into the condyle Avulsion fracture |
Axial stress, stability from the contralateral alar ligament and tectorial membrane Stability from the intact alar ligament and tectorial membrane Tear of the bony attachment of the alar ligament. Instability due to associated injuries of the tectorial membrane |
|
IVA
IVB |
OCF + clivus avulsion fracture
OCF + clivus fracture |
Unstable
Highly unstable |
CONCLUSION
Bilateral OCF associated with inferior clivus separation fractures remain a very rare phenomenon. We propose a novel type of fracture of the Anderson and Montesano classification system with two further anatomical sub-types. Type IVA occurs when OCF is associated with a clival avulsion fracture whereas type IVB is associated with a ‘en piece’ separation of the clivus. We hope this knowledge can guide spine surgeons towards successful management of these potentially devastating injuries.
REFERENCES
1. Bell C. Surgical Observations. Middlesex Hosp J. 1817; 4: 469-470.
13. Maserati MB, Stephens B, Zohny Z, Lee JY, Kanter AS, Spiro RM, Okonkwo DO. Occipital condyle fractures: clinical decision rule and surgical management. J Neurosurg Spine. 2009; 11: 388–395.
17. Fuentes S, Bouillot P, Dufour H, Grisoli F. Occipital condyle fractures and clivus epidural hematoma. Case report. Neurochirurgie. 2000; 46: 563–567.









































































































































