An Unnerving Cause of Hand Pain
- 1. Inova Fairfax Medical Campus – Fairfax Family Practice Sports Medicine Fellowship Program, USA
ABSTRACT
Anatomical variations, such as a bifid median nerve, have been reported as potential contributing factors for the development of carpal tunnel syndrome (CTS). These anomalies are typically diagnosed intraoperatively. With the growing use of sonography as a diagnostic tool, the prevalence of bifid median nerves has increased from 2.8% to 15.4-19%. We report on a case of CTS in an individual with a bifid median nerve and an accessory flexor digitorum superficialis indicis bisecting the two divisions of the median nerve that was diagnosed with sonography. Use of sonography can aid in procedural management of patients with CTS.
KEYWORDS
Bifid median nerve; Carpal tunnel syndrome; Ultrasound; Anatomic anomaly; Musculoskeletal ultrasound; Neuromuscular sonography; Sonology.
CITATION
Ho G, Macomb C, Stuek S (2022) An Unnerving Cause of Hand Pain – Carpal Tunnel Syndrome with Accessory Flexor Digitorum Superficialis Indicis interposing a Bifid Median Nerve. Ann Sports Med Res 9(1): 1187.
ABBREVIATIONS
CTS: Carpal Tunnel Syndrome; GE: General Electric; D5: 5% Dextrose; cm: Centimeter; mm2 : Millimeter squared; ml: Milliliter; mg: Milligram; SAX: Short-axis; LAX: Long-axis; CSA: Cross-sectional area; EMG: Electromyography.
INTRODUCTION
Carpal tunnel syndrome is the most common entrapment neuropathy diagnosed in the outpatient setting, often secondary to lifestyle or work-related repetitive activities of the hand and wrist; systemic illnesses such as diabetes mellitus, hypothyroidism, and rheumatoid arthritis; or otherwise considered idiopathic [1]. In addition, the surgical literature has increasingly reported on anatomical variations as potential underlying contributing factors for the development of carpal tunnel syndrome [2-6]. Lanz [7] further classified these anatomical variations into four separate categories where high division of the median nerve is an uncommon variation that is in category three. High division of the median nerve was initially reported at 2.8% by Lanz10, but has been more frequently reported with a prevalence of 15.4-19% with the growing use of sonography as a diagnostic tool in the diagnosis of carpal tunnel syndrome [8,9].
We present a case of carpal tunnel syndrome in an individual with a high division of the median nerve – the so-called bifid median nerve – with an accessory flexor digitorum superficialis indicis bisecting the two median nerve divisions.
CASE PRESENTATION
A 58-year-old left-hand dominant female, with a history of bilateral rotator cuff tendinopathy, presented with numbness in the first three digits of her left hand for the past few months. Her symptoms were gradual in onset, without a history of injury or trauma. The patient reported that the numbness is intermittent and worse at night. She occasionally experienced radiation of her symptoms to the volar aspect of the mid-forearm. The patient noted difficulty holding a pen after a period of time, but otherwise denied other overt signs of weakness. The patient denied neck pain. During her initial evaluation, her physical examination demonstrated a positive Tinel’s sign over the median nerve at the carpal tunnel – and to a lesser extent over the pronator teres – with globally normal muscle strength testing and sensation to light touch. No thenar muscle atrophy was noted. Conservative treatment for carpal tunnel syndrome was recommended at her initial encounter. At follow up, the patient reported adherence to nerve glide exercises, nighttime splinting, and activity modification without significant relief of her symptoms. Her physical examination at follow up demonstrated reproduction of her symptoms with manual percussion over the carpal tunnel, but no longer had any findings over the pronator teres.
A musculoskeletal and neuromuscular ultrasound was performed using a General Electric (GE) NextGen Logiq e R8 ultrasound machine and L4-12t-RS linear transducer (GE Healthcare; Chicago, IL, USA). Grey-scale imaging showed a bifid median nerve at the level of the carpal tunnel inlet, with crosssectional areas measuring 22mm2 and 5mm2 of the radial and ulnar divisions, respectively (Figure 1).
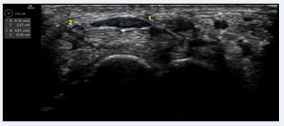
Figure 1 Short-axis (SAX) view of a Bifid Median Nerve in the carpal tunnel inlet under ultrasound. Note the smaller ulnar sided division (2) of the median nerve with its cross-sectional area (CSA) measuring 5mm2 and the larger radial division (1) of the nerve with a CSA of 22mm2 .
An interposing muscle slip – identified as an accessory flexor digitorum superficialis muscle – was noted between the two divisions of the median nerve proximal to the transverse carpal ligament (Figure 2,
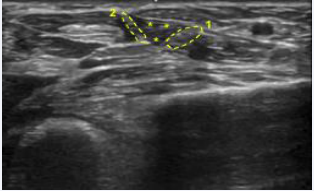
Figure 2 Short-axis (SAX) view of Bifid Median Nerve (- - -) and Accessory Flexor Digitorum Superficialis Indicis (***) over the pronator teres, proximal to the carpal tunnel inlet under ultrasound. Note the ulnar (2) and radial (1) divisions of the median nerve, interposed by the accessory muscle.
Figure 3.
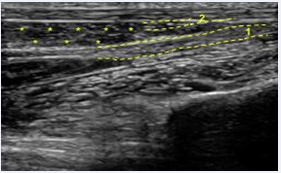
Figure 3 Long-axis (LAX) oblique view of Bifid Median Nerve (- - -) and Accessory Flexor Digitorum Superficialis Indicis (***) over the pronator teres, proximal of the carpal tunnel inlet under ultrasound. Note the smaller ulnar (2) and larger radial (1) divisions of the median nerve, interposed by the accessory muscle.
This muscle was scanned and found to have a distal insertion at the middle phalanx of the index finger. Of note, a persistent median artery was not evident on power doppler imaging within the boundaries of the carpal tunnel or over the pronator teres. Survey images of the thenar muscles were normal without findings to suggest denervation sequelae.
An ultrasound guided perineural injection of an 11-ml solution containing triamcinolone acetonide, 5% dextrose (D5) and local anesthetic was performed to both divisions of the median nerve using a 25-gauge needle (Figure 4).
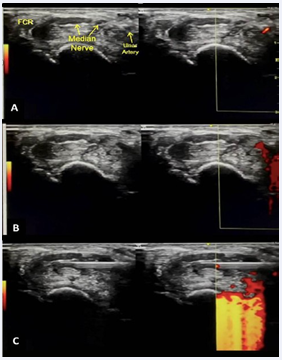
Figure 4 Ultrasound-guided injections of the bifid median nerve. (A) Short-axis (SAX) view of the Bifid Median Nerve under ultrasound guidance prior to injection; note doppler positivity of ulnar artery on the right image. In-plane needle guided injection of the ulnar (B) and radial (C) divisions of the bifid median nerve from ulnar-to-radial direction above (volar) and below (deep, dorsal) each nerve division.
The components of the injected solution were 1 ml of 40 mg/ml of triamcinolone acetonide, 2 ml of 1% lidocaine hydrochloride without epinephrine, 1 ml of 50% dextrose, and 7 ml of sterile water. Under continuous grey-scale and power Doppler imaging, a short-axis (SAX) view of the bifid median nerve was imaged, noting Doppler positivity of the ulnar artery. In-plane needle guidance from an ulnar-to-radial direction was performed to avoid the ulnar artery and nerve. Perineural injection of the ulnar and radial divisions of the bifid median nerve was accomplished above (volar) and below (deep; dorsal) each nerve division. The patient reported 100% relief of symptoms immediately following the procedure. At one month follow up post-procedure, the patient reported complete resolution of her symptoms.
DISCUSSION
Anatomic variations of the median nerve have long been described in the literature, being first classified by Lanz in 1977 [7].With the growing use of point-of-care diagnostic sonography, high divisions – or bifid – median nerves are being increasingly recognized. The estimated prevalence of a bifid median nerve has increased from 2.8% to 19% with ultrasound [8,12]. A bifid median nerve has been reported as a potential risk factor for the development of carpal tunnel syndrome, due to the nerve’s increased cross-sectional area compared to a non-bifid nerve and its resulting increased occupancy within the carpal tunnel [8]. When present, a bifid median nerve is often accompanied by a persistent median artery [14,13,7], and on rare occasions has been associated with an aberrant muscle. Our patient presents a rare clinical finding of an accessory flexor digitorum superficialis indicis bisecting the bifid median nerve without a persistent median artery, contributing to clinical symptoms of carpal tunnel syndrome.
The flexor digitorum superficialis indicis has been described as an accessory muscle of the hand and wrist usually encountered during operative procedures in patients with symptoms of carpal tunnel syndrome, with the muscle noted to displace or compress the median nerve [2-4,10,11]. Our literature review yielded only one other case report where a flexor digitorum superficialis indicis has been associated with penetration of the median nerve. Skie and Ciocanel [11] described this finding during an operative procedure in a patient who presented with carpal tunnel symptoms but had a conduction delay 4 cm proximal to the wrist crease on EMG. Intraoperatively, the flexor digitorum superficialis indicis penetrated the median nerve which was divided into a deep component – making up two-thirds of the total nerve diameter – and a superficial component that was one-third of the total diameter. The median nerve was noted to conjoin proximally and distally to the penetrating flexor digitorum superficialis indicis [11] Unlike the case reported by Skie and Ciocanel [11] – which was diagnosed intraoperatively – the accessory muscle in our case was observed non-invasively under sonography. Additionally, our nerve was considered a bifid median nerve as the divisions did not rejoin distally as it did in the case reported by Skie and Ciocancel [11]
Our case highlights the value and utility of ultrasound as a diagnostic and therapeutic tool in the management of peripheral neuropathies. Ultrasound can be performed in a number of settings and is an accurate, cost-effective method for the anatomic evaluation of entrapment neuropathies. Sonographic criteria for the diagnosis of carpal tunnel syndrome has been well described and correlate with well-established diagnostic modalities, such as electrodiagnostics [15,11,13,18]. Understanding the anatomical course of the median nerve is important for procedural management of patients with carpal tunnel syndrome. If symptoms become refractory to percutaneous interventions,these sonographic findings may be critical to aid in surgical planning and intervention, and ultimately playing key roles in the prevention of intraoperative and perioperative complications.
CONCLUSION
We present a rarely reported case of carpal tunnel syndrome with an accessory flexor digitorum superficialis indicis, bisecting a high division, bifid median nerve, diagnosed non-invasively with sonography. In addition to highlighting the clinical utility of the diagnostic modality, we report on the successful short-term outcome of an ultrasound-guided percutaneous intervention in our patient.









































































































































