A Case of Ischial Bursitis Occurring in Obturator Externus Muscle Injury in Professional Football Player
- 1. Department of Radiology University of Insubria, Italy
- 2. Department of Biomedicine, Neuroscience and Advanced Diagnostics (Bi.N.D.), University of Palermo, Italy
- 3. Department of Radiology University of Insubria, Italy
- 4. Department of Sport, Medicine Ospedale di Circolo e Fondazione Macchi, Italy
- 5. 4 Department of Sport Medicine, Milan Lab, Italy
- 6. Department of Sport Medicine, Milan Lab, Italy
- 7. Department of Sport Medicine, Milan Lab, Italy
Abstract
The obturator externus muscle plays an essential role in hip stability. In professional athletes early diagnosis in case of injury is important to allow a quick return to sporting activity.
A 25-year-old high-level professional football player suffered an obturator externus muscle injury during an official match for which he under went multiple MRI examinations in recovery period.
A type 3 muscular injury was observed and studied: during subsequent checks, the lesion showed physiological repair phenomena but allowed to highlight the presence of a bursal collection of the obturator externus at the ischiatic insertion of the muscle.
This type of bursa of the obturator externus muscle has never been described in the literature both in cadavers and in vivo patients. Identifying this type of bursitis in professional soccer players in case of obturator externus injury is essential to avoid prolonged hip pain and excessively long recovery time.
Keywords
Obturator externus, Bursa, Professional athletes, Muscular injury, Hip
Citation
Gatta T, Greco A, Lamantea S, Calvi M, Mazzoni S, et al. (2023) A Case of Ischial Bursitis Occurring in Obturator Externus Muscle Injury in Professional Football Player. Ann Sports Med Res 10(2): 1204.
INTRODUCTION
The obturator externus muscle is a flat skeletal muscle located in hip area.
This muscle originates from the external edge of the obturator foramen. From their origin fibers head laterally, superiorly and posteriorly, surround the coxo-femoral joint and are inserted with a common terminus in the trochanteric fossa [1]. It relates anteriorly with the iliopsoas, pectineus, gracilis, adductor brevis and major muscles, with the femoral neck and with the joint capsule. It also arises anterior to the obturator membrane and the quadratus femoris muscle. Its innervation is provided by the obturator nerve (L1-L4) [2].
Its main function is to rotate and abduct the hip, as well as stabilize hip joint when walking. It is also involved in stabilizing other joints of the lower limb and torso [3].
Since it is an hip’s deep muscle it is infrequent to identify and diagnose an injury, indeed few cases are reported in literature [4].
Although obturator externus injury in football players is an uncommon finding, the importance of a correct and prompt diagnosis about lesions of the obturator externus appears particularly relevant when it occurs in professional athletes, as it can lead to a prolonged absence from sporting activities [5].
Magnetic resonance imaging (MRI) represents the gold standard examination for identifying muscular lesions and defining their characteristics [6], as well for determining recovery time [7].
CASE PRESENTATION
A 25-year-old high-level professional athlete from main football league get injured during an official match, resulting in pain in the anterior region of his left thigh.
The next day he underwent an MRI diagnostic examination. All images were obtained using a 1.5-Tesla magnet system (Philips Ingenia Ambition/Elition). The examination was performed through coronal and axial plane acquisitions, integrated with DWI sequences and 3D reconstructions (DWIBS).
The exam highlighted extensive signal alteration of the left obturator externus muscle that almost completely affects the entire muscular element. This signal hyperintensity was expression of interstitial hemorrhage between tertiary fibers, associated with edema. In central area the hyperintensity had an inhomogeneous appearance and the signal had a slightly reduced intensity for an extension of about 24 mm, expression of real muscle damage. Signal alteration also affected the adjacent margin of obturator internus muscle, by contiguity. In DWI acquisitions, a reduction of diffusivity involving the muscle was observed (Figure 1).
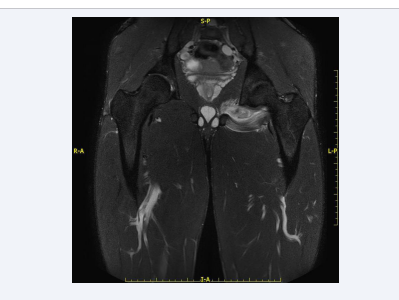
Figure 1: MRI coronal STIR TSE weighted image shows signal alteration of the entire obturator externus muscle, (type 3 lesion).
These findings were expression of a type 3 lesion of the obturator externus, without serum-blood collection, with marginal peripheral involvement of the obturator internus.
One week after, the patient underwent a second MRI examination which showed, in DWI acquisitions, significantly reduction of the diffusivity narrowing, both in terms of extension and signal, with residual diffusivity reduction only in the most medial portion of the left obturator externus, expression of resolution of the interstitial hemorrhage. There was persistence of edema in the same site, however less extensive than in previous investigation (Figure 2a).

Figure 2: Axial T2 (a) and coronal STIR TSE weighted (b) acquisitions of the second MRI examination (after seven days) demonstrate the resolution of the interstitial hemorrhage, with low persistence of edema, and highlight the appearance of a bursal collection at the ischiatic insertion of the muscle, with “drop” morphology.
Compared to the previous investigation, effusion with a “drop” morphology appeared at ischiatic insertion of the obturator externus. The effusion had a weak hypersignal in SE proton density acquisitions, expression of hemorrhagic component. The effusion had clear margins, well delimited interface towards to the muscle and to the bone, however free of spongious edema.
This last finding might be expression of a bursal collection of the obturator externus (Figure 2b).
The last checkup was executed two weeks after the injury and demonstrated further reduction of the residual narrowing of diffusivity. In T2 acquisitions with fat suppression persisted hypersignal, lower than in previous investigations, involving only the obturator externus muscle. The signal alteration mainly affected the medial portion of the muscle. The hypersignal described at the obturator internus appeared completely resolved (Figure 3a).
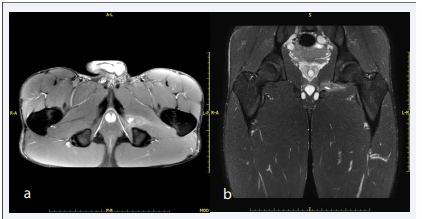
Figure 3: Axial T2 (a) and coronal STIR TSE weighted (b) acquisitions of the last MRI examination show minimal residual hypersignal only in the medial portion of the muscle and significant reduction of bursitis.
Even the effusion described in previous investigation appeared considerably reduced, with an extension of just over 10 mm, with loss of the teardrop morphology previously described (Figure 3b). The scans obtained after intravenous infusion of paramagnetic contrast medium showed homogeneous contrast enhancement of the obturator internus muscle, in contrast with the markedly reduced signal in T2 acquisitions, expression of reparative colonization of the interstitial component between tertiary fibers of the muscle.
Therefore after the last examination, about four weeks after injury, the athlete began a gradual return to training without complications and clinical manifestations.
DISCUSSION
Muscle injuries are one of the main trauma that occurs in athletes [8].
These lesions can be distinguished in functional lesions, which may not be detectable with diagnostic tests, or structural lesions, that present macroscopic evidence at US or MRI imaging [9].
For structural lesions, MRI represents the gold standard diagnostic test, as it allows to characterize the lesion in terms of location, type, size, timing and anatomical characteristics [10].
Several studies suggest classifying injuries in terms of: structural component (muscle, joint and tendon), localization (intramuscular, myofascial, perifascial, musculotendinous), affected muscle area (proximal, middle and distal) and severity [11]
According to the Mueller-Wohlfahrt classification, structural muscle injury can be divided into two classes: type 3 which involves a partial muscle injury and type 4 which implies a subtotal or total injury. Particularly type 3 can be distinguished in 3A, or rather minor partial lesion in which there is lesion of one or more primary bundles within a secondary bundle, and 3B, or modest partial lesion in which there is lesion of one secondary bundle with breaking surface less than 50% of the muscle surface. Type 4 injury instead involves a subtotal or total tear or tendon avulsion in which the lesion affects more than 50% of the muscle surface, all of the muscle or the tendon-bone junction [9].
Although lesions of the obturator externus muscle are quite rare in general population, they appear to be predominantly frequent in elite soccer players. This explains why it is important to suspect them when the athlete shows pain in the hips and in the anterior region of the thighs, since a lesion of hip’s deep muscles can lead to delayed functional recovery and prolonged withdrawal from sporting activity [12].
The physiological evolution of the lesion explained in our case report also allowed us to highlight the presence of a synovial bursa pertaining to the obturator externus muscle, in which the hemorrhage that initially occurred between the tertiary fibers of the muscle has drained.
Numerous synovial bursae have been identified within the body [13], which are serous bursae composed of small sacs of synovial fluid located within joints. Their main function is to provide protection to joint structures which are subjected to friction and also allow a distribution of joint loads, which allows for greater fluidity in movement [14]. Pathological phenomena affecting the bursae can be inflammatory, infective or hemorrhagic phenomena, arising following trauma involving adjacent muscles [15]. Indeed blood or serous effusion can flow out inside the bursa with consequent local irritation and symptoms such as pain and stiffness, which can occur both at rest and during movement [16].
There are very few cases in the literature describing the existence of a synovial bursa of the obturator externus muscle.
Specifically there is a single review of Kassarjian et al demonstrating the communication between the obturator externus bursa and the hip joint based on the use of MRI arthrography [17].
A further study reported by Robinson et al illustrates the observation of obturator externus bursa in 8 dissected cadavers and in 10 patients who underwent MRI imaging; also in their analysis, in all patients, the bursa locates in communication with the hip joint [18].
In our case report the obturator externus muscle bursa is located at the interface with the ischium. Unlike the few previous studies that have dealt with this anatomical relief, it is the first time that this location has been observed, indeed in the available literature only cases of bursa located on the side of the hip joint, both in vivo and in cadavers, are reported.
CONCLUSION
In conclusion in our case report we have reported an anatomical variation not yet observed in the literature; furthermore our finding, in agreement with previously quoted studies, demonstrate that injuries of the obturator externus and associated bursitis may represent a major pain point of the hip joint and that it is therefore worthy of suspicion and of in-depth study, particularly in subjects predisposed to this type of injury, such as high level athletes.
ACKNOWLEDGEMENTS
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by and The first draft of the manuscript was written by and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
REFERENCES
4. Rhim HC, Gureck AE, Jang KM. Acute Obturator Externus Injury in Professional Soccer Players: A Case Series.
5. Medicina (Kaunas). 2022; 58: 1145.
14. Bywaters EG. THE BURSAE OF THE BODY. Ann Rheum Dis. 1965; 24: 215-218.
16. Khodaee M. Common Superficial Bursitis. Am Fam Physician. 2017; 95: 224-231.








































































































































{kind=link}