Bilateral Acute Myotendinous Rupture of the Rectus Abdominis Muscle
- 1. Department of Emergency Medicine, Radboud University Medical Center, Netherlands
- 2. Department of Trauma surgery, Radboud University Medical Center, Netherlands
Abstract
Background: Rupture of the rectus abdominis muscle is a rarely seen condition.
Study Design: Case report with review of the literature.
Case: A 24 year old woman sustained a partial rupture of the rectus abdominis muscle after a simple workout.
Methods: MEDLINE, PubMed and Cochrane databases search.
Conclusion: Rupture of the rectus abdominis muscle is a rare condition which can occur after minor activity. Ultrasound (US) and Magnetic Resonance Imaging (MRI) are good diagnostic methods to identify the specific rupture side. Therapy depends on the extensiveness of the rupture. In case of intact fascia, conservative treatment is considered the best management.
Keywords
Rectus abdominis muscle , Rupture , MRI , Conservative treatment
Citation
Cottaar M, van Rooijen S, Doomernik D, Tan E (2016) Bilateral Acute Myotendinous Rupture of the Rectus Abdominis Muscle. Ann Sports Med Res 3(2): 1061.
INTRODUCTION
The rectus abdominis muscle is a paired muscle group in the abdominal wall, separated by the linea alba in the midline. It originates at the xiphoid process and the costal cartilages of ribs V to VII; its insertion is at the pubic symphysis [1].Three bands of connective tissue, called the intersections tendinae, divide both parts of the rectus abdominis muscle in eight distinct muscle bellies. The function of this muscle is to pull the ribs towards the pelvis, thereby resulting in flexion of the lumbar spine. It also assists with breathing, coughing and provides a muscular wall to keep the internal organs intact en creating intra-abdominal pressure.
Muscle strains or ruptures normally occur in muscles that cross multiple joints or have complex architecture, e.g. the hamstring, the rectus femoris, gastrocnemius muscles and adductor longus muscles [2]. These injuries are the result of contraction and extensive stretching. Therefore a rupture of the rectus abdominis muscle is a rarely seen condition.
So far, rupture of the rectus abdominis muscle is only described in a few cases with abdominal trauma, in elite sports players or during infections, in which lung infections are the most frequent [3-7].
The aim of this study is to compile the known literature, and thereby providing a complete overview for this topic.
CASE
A 24 year old woman was admitted to the Emergency Department (ED) with acute abdominal pain. During a routine weekly workout of the abdominal muscles in a fitness centre she experienced a sharp pain underneath the umbilicus. The workout consisted of an exercise in which she laid on her back on the floor and raises both legs in an extended position. Another person pushes the legs back down, to create a strain on the rectus abdominis muscle. The pain occurred while somebody pushed her legs downwards as described before.
In the ED she was unable to extend her legs or to lie down. The pain was given a 9 on the Numeric Rating Scale (NRS). The patient’s history showed daily usage of corticosteroids (50 µg salmeterol/ 500 µg fluticasone) and sporadic use of 100 µg salbutamol since childhood because of asthma, and prednisone once in preparation of spondylodesis of her lumbar spine (L5- S1). Moreover, she was using a Nuvaring (ethinylestradiol/ etonogestrel). No previous abdominal operations, pregnancy or allergies were reported. On average she performs abs workout on a weekly basis without any previous problems.
At physical examination we saw a woman in pain, despite analgesia with morphine. Abdominal inspection showed no signs of hernia or hematoma. Peristalsis was present and no palpable mass or dell was felt. The abdomen was extremely painful to palpation in the region below the umbilicus.
In the differential diagnosis a strangulated abdominal hernia was considered.
An ultrasound (US) of the lower abdomen was performed, to see whether there was a herniation of the abdominal wall, a rectus hematoma, or even a rupture of the abdominal muscle.
The US showed a partial rupture of the rectus abdominis muscle at both sides of the linea alba (Figures 1-3).
The rupture was approximately 1cm wide and 0.6cm deep. At the ventral side of the abdominal wall, muscle fibers were undamaged and the linea alba was intact. No intramuscular hematoma was seen.
Because of this rare finding and no adequate response to standard pain medication, the patient was admitted to the surgical department for observation and pain management. The next day, the patient was discharged home with an adequate pain regime and physiotherapy, consisting of an abdominal bandage to provide pressure in the affected place and a normal mobilization programme under supervision of a physiotherapist.
One week after discharge an MRI was performed to investigate the rupture in detail (Figures 4-6).
The MRI showed fluid in the right and left rectus abdominis muscle, with almost complete rupture of the muscle fibers. The fascia and linea alba were intact. Because of the intact fascia the conservative treatment with physiotherapy and pain medication

Figure 1: Rupture in the right abdominal muscle.
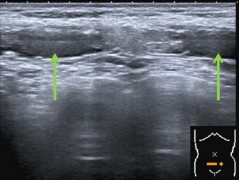
Figure 2: Rupture in both abdominal muscles.

Figure 3: Rupture in the left abdominal muscle.
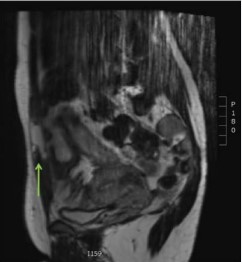
Figure 4: MRI T2, Coronal view of the right abdominal muscle.

Figure 5: MRI T2, Sagittal view of the abdominal muscle.
was maintained. Follow up after 2, 6 and 11 weeks consisted of a visit to the outpatient clinic and an appointment with the doctor (author ET) who saw her during her initial visit to the ED and was uneventful. The patient started working out 10 weeks after the event without any problems.

Figure 6: MRI T2, Axial view of the abdominal muscle.
SEARCH
A search was conducted to identify reports in which rupture of the rectus abdominis muscle was described, using the MEDLINE, Embase, PubMed and Cochrane databases. The following MeSH terms were used: “rectus abdominis” and “rupture”. They were also used as free text. These terms were applied in various combinations in addition to the use of the ‘related articles’ and ‘citing articles’ function.
This resulted in a total of 24 hits. Full-text articles were studied on restriction of language of publication (English and Dutch) and manual cross-referencing was performed. A total of 15 articles were identified and used for the literature review.
LITETATURE REVIEW
Rupture of the rectus abdominis muscle was first described in 1943 as a complication of pregnancy [8]. After that, a few more case reports were reported where infectious diseases and blunt abdominal trauma are described as a risk factor for developing rupture of the rectus abdominis muscle [9-16]. Since 1987, only one additional report on rupture of the rectus abdominis muscle was published [15].
Rupture of the rectus abdominis muscle can be divided in two classes: (1) direct; (2) indirect.
In direct injury one may think of blunt abdominal trauma, like crush injury, high velocity road traffic accident or bicycle accidents [14-16].
Indirect injury, like coughing, is described mainly in elderly patients suffering from infectious disease [9, 11].
When examining a patient with acute abdominal pain at the Emergency Department, one should have a broad differential diagnosis. Besides the most common diagnosis, like appendicitis, diverticulitis or a twisted ovarian cyst, the treating physician should also consider a rupture of the rectus abdominis muscle, as this can occur after minor strain on the muscle, or a rectus hematoma [9,11,17]. Another rare diagnosis one should consider is the syndrome of the rectus abdominis muscle [18]. It is a disorder of unknown etiology that produces rupture or tears of the epigastric artery and stretches the rectus cutaneous medialis nerve, producing excruciating pain. This disorder is misdiagnosed in 60-93% of the cases, resulting in unnecessary invasive procedures. Insertion of 5ml 1% lidocaine can be a useful, and simple, diagnostic for this syndrome.
Lidocaine can also be helpful in the diagnosis of Anterior Cutaneous Nerve Entrapment Syndrome (ACNES) [19].
In the ED the rupture was diagnosed by US. Compared to MRI, US is less invasive, well tolerated and cost-effective [20-21]. In contrary, its contrast is not as good as MRI.
Therefore an MRI was performed in a later stage, to establish the extent of the rupture.
DISCUSSION
This case describes the rare occurrence of rupture of the rectus abdominis muscle after minor activity. Transection of the rectus abdominis muscles due to trauma, elite sports, pregnancy and infectious diseases has been reported in literature; however the cause of rupture after minor activity remains unknown.
A possible explanation for the spontaneous rupture in our case is the daily usage of corticosteroids since childhood.
Corticosteroid induced myopathy is a well-known side-effect of systemical corticosteroid use which might be an initiating factor of muscle rupture [22-25]. In skeletal muscle, systemic glucocorticosteroids, eg. prednisone, decrease the rate of protein synthesis and increase the rate of protein breakdown contributing to atrophy.
The dose inducing myopathy varies greatly among patients. Typically a dose given of less than 10mg/day is rarely associated with glucocorticosteroid induced myopathy. A dose of a topical inhaled glucocorticosteroid is less then 10mg/day (eg 200mcg per dose), so glucocorticosteroid induced myopathy is not likely to develop.
There are no reports of a relation between topical glucocorticosteroids, such as the fluticasone used in this case, and muscle ruptures.
Until now, the relevance of the length of corticosteroid therapy to muscle injury is only described in rat models [26]. They describe that muscle atrophy is possibly induced by the upregulation of myostatin expression through a glucocorticoid receptor-mediated pathway.
A correlation between the dosage combined with the length of usage is not described in literature.
In almost all known cases of muscle rupture, conservative treatment resulted in a good outcome [21]. Known indications for surgery are muscle ruptures with large hematomas in athletes, a complete (III degree) strain or tear of a muscle with few or no agonist muscles, or a partial (II degree) strain if more than half of the muscle belly is torn [27].
Based on the known pathobiology of muscle regeneration and the intact fascia, conservative treatment with physiotherapy and medication against the pain was the treatment of choice.
One clear limitation of this study is that it consists of a single case report. Follow up consists of three months. At the time of the ED visit, we did not draw blood samples to determine whether there were any coagulation disorders, as there was no clinical suspicion. During follow up we also had no indication to look further for connective tissue diseases or other metabolic disorders, since the patient did not report any other health problems.
CONCLUSION
In the case of extreme pain sub umbilical after abs exercises or workout, not only rectus hematoma but also rupture of the rectus abdominis muscle should be included in the differential diagnosis.
This case report gives an overview how to diagnose and treat a rupture of the rectus abdominis muscle. Spontaneous rupture of the rectus abdominis muscle is a rare condition with unknown underlying pathology. In the emergency setting US is a good diagnostic method. The extent of the rupture can be defined later by MRI. Therapy depends on the extensiveness of the rupture. In case of intact fascia, conservative treatment is a well-established option.
REFERENCES
1. Tillmann BN. Atlas van de menselijke anatomie. 2008.
2. Garrett WE. Muscle strain injuries. Am J Sports Med .1996; 24: S2-8.
3. Metzdorff MT, Miller SH, Smiley P, Klabacha ME. Ann Plast Surg. 1984; 13: 63-66.
11. Horsburgh AG. Rupture of the rectus abdominis muscle. Br Med J. 1962; 2: 898.
12. McCarthy D, Durkin TE. Rupture of the rectus abdominis muscle. Br Med J. 1963; 1: 58-59.










































































































































{kind=link}