Does the Body Fat Mass Interfere on the Pain Tolerance From Attack Techniques at the Abdominal Region of Karate Athletes?
- 1. Euro American University Center Brazil
- 2. Euro American University Center Brazil
- 3. Euro American University Center Brazil
- 4. University of Brasília, Brazil
- 5. University of São Paulo, Brazil
- 6. Euro American University Center Brazil
Abstract
The ability to tolerate pain can influence the physical performance of several sports. This study compared the pain tolerance to attack techniques impacting the abdominal region of karate athletes from different profiles. The sample was 25 men karate athletes of black belts of Uechi-Ryu (32.71 ± 8.22 years, 82.45 ± 9.92 kg, 1.77 ± 0.05 m). The volunteers performed three visits, first for sample selection, second visit for anamnesis, body composition and familiarization with tolerability test, and third visit, tolerability test. The volunteers were divided into two groups: G1 with fat percentage < 23%; G2 with fat percentage > 23%. Total body mass (TBM), absolute and relative muscle mass [MM (kg) and MMR (%)], absolute and relative fat mass [FM (kg) and FMR (%)] were assessed. Differences were identified between G1 and G2 in TBM, MMR, FM and FMR (p = 0.001). Pain tolerance was similar between groups (p = 0.36), with FMR weakly correlated with the number of blows received (r = 0.22). In conclusion, body fat does not interfere with pain tolerance induced by abdominal punches in experience karate athletes.
Keywords
• Pain
• Martial Arts
• Body Composition
CITATION
de ALMEIDA LR, de Araújo SILVA JG, PEREIRA LC, LAGE V, CANESTRI R, et al. (2023) Does the Body Fat Mass Interfere on the Pain Tolerance From Attack Techniques at the Abdominal Region of Karate Athletes? Ann Sports Med Res 10(4): 1216.
INTRODUCTION
In some Eastern martial arts, specific training methods were developed with the objective of providing practitioners with the understanding and learning of pain tolerance through techniques ranging from amortization to meditation [1,2]. In Japanese martial arts, more specifically karate, this type of training consists of body use or instruments to prepare the fighter for combat. This process of preparation of the body involves desensitization techniques of some regions, with the goal of altering the tolerance of pain among those involved [3].
Pain is a complex and multifactorial phenomenon that is simultaneously associated with sensory/discriminative, emotional/affective, and evaluative/cognitive aspects, being considered a personal, subjective experience, influenced by previous experiences, psychophysiological and sociocultural factors [4,5]. For the National Institute of Health (NIH), the most reliable indicator of pain intensity is self-assessment, with the Numerical Rating Scale (NRS) being the most commonly used scale for pain assessment [6]. The International Association for Study of Pain (IASP) characterizes pain as an unpleasant sensory and emotional experience associated with or like that associated with actual or potential tissue damage [7]. The time in which the stimulus is repeated causes the perception of pain to change [8]. Studies have demonstrated that the magnitude of the individuals’ resistance to pain depends on their previous experiences [9,10], body structure and intensity of the stimulus delivered [6,11], as well as their psychological profile, age, and gender [12,13].
In terms of body structure, the body composition is considered one of the main markers of athletic performance of karatecas of different styles and categories [14]. For example, a negative association between body fat mass and karate specific aerobic test performance was shown [15]. But it is hitherto not well understood if body composition, specifically the fat component, influences the sensation of physical impact imposed by martial techniques (MT) like punches, for instance, whether body adiposity to interfere the pain tolerance (PT) induced by MT thrown by an opponent in a simulated fight situation. According to practical knowledge, athletes with a higher fat mass better tolerate pain induced per traumatic MT thus allowing them to support a greater number of repetitions, especially at abdominal region because of the reduced bony envelope of the anterior cavity. Therefore, one would have greater resistance to MT compared with individuals of smaller body fat mass. That said, the question that emerges is: does fat mass really interfere on pain tolerance of karate athletes?
Therefore, the aim of this study was to compare pain tolerance in the abdominal region between karatecas with different percentages of body fat. We hypothesize that the subjects with higher percentage of body fat support a higher number of abdominal striking techniques.
METHODS
This was a cross-sectional study design that followed the guidelines proposed by resolution 510/2016 of the National Health Council, being approved by the Research Ethics Committee of the Euro American University Center (253.531/2019).
Participants
Black belts of Uechi-Ryu karate athletes volunteered to take part in this study, after signing a free and informed consent form. They had at least six years of experience in the modality, practicing uninterruptedly when the study was conducted. Participants presented no cardiovascular and/or osteomyoarticular restrictions, after answering the PAR-Q survey. All the selected participants completed the three stages of the study, according to the experimental design presented in (Figure 1). The sample was stratified into groups according to relative fat mass, where G1 ≤ 23% (Low %Fat) and G2 ≥ 23% (High %Fat).
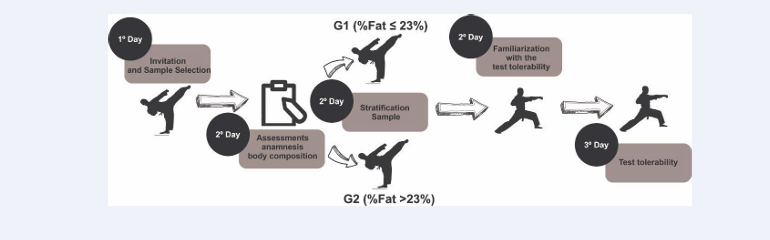
Figure 1: Flowchart of hierarchical processes of data collection.
Anthropometric measurements and body composition
Height was measured using the stadiometer (SECA, 206) with an accuracy of 1.0 mm and was measured in an orthostatic position, without shoes, with the feet together and heels, gluteus, and occipital region in contact with the interface of the measurement scale. The evaluation was made using the Frankfurt Plan, where a line parallel to the ground is drawn, intersecting the auditory method and the lower edge of the ocular orbit. The measurement was performed at the end of a complete inspiration followed by a voluntary respiratory inhibition [16].
Total body mass (TBM), absolute [MM (kg)] and relative [MMR (%)] muscle mass; as well as absolute [FM (kg)] and relative [FMR (%)] fat mass were measured. For this, the Bioimpedance device (HBF 514C, OMRON) with a scale of 0.1 kg and 0.1% body fat was used. For the bioelectric impedance method, participants were instructed to wear bathing suits and abstain from food and water consumption for at least 4 hours, physical activity for 12 h, alcohol consumption for 48 h, and tonot use diuretics within 7 days prior to the evaluation. The circumference of Waist (cm) was measured through the anthropometric technique, where the point of smallest abdominal circumference using a tape measure (T87, WISO) was delimited. Both techniques guided the body composition and division of the sample groups. They were referred to urinate approximately 30 minutes before collection, as recommended by the manufacturer [17]. The feet were positioned centrally in the pruning electrodes, to distribute the weight evenly on the platform and the flexed shoulder parallel to the ground wielding the electrodes of the display unit. The appropriate time indicated by the scale was then waited for the complete measurement of the data.
Pain Tolerance Protocol
The pain tolerance verification protocol followed the chronological order of 1st Stage - Familiarization; 2nd Stage – Warm-up; and 3rd Stage - Striking and pain verification. The first stage was applied on different days of steps 2 and 3. In the familiarization stage, 2 volunteers hereby called issuing agents (emitters) were selected to perform the strokes techniques on their peers. This choice was decided upon by aspects such as: availability of time and involvement with the study. They attended demonstrations and received guidance/explanations about technical positions for data collection and co-responsibility. Then, a technical session was started, with the whole sample, where the blows were delivered with submaximal intensity, to calibrate the accuracy of the blows and the understanding of the protocol by those who would receive the techniques. The emitters throw the technique of punch the receiver with grade/intensity 3 according to the Numerical Estimation Scale (NRS, 0-10). At this initial moment, 10 blows were performed (abdominal punch technique). The total number of punches was based on previous pilot test that allowed us to conclude that this total is easily tolerable among subjects with the sample characteristics. To prevent residual emitter fatigue, each subject performed the test on two volunteers per data collection shift, separated by a 60-minute rest interval as well as each emitter working only with the volunteers of its anthropometric group.
To define and equalize the strength-power of the upper limbs among the emitter of each group, the 9 kg Medicine Ball Throwing Test (MB) was used. The throw started from the sit down position comfortably on the bench tilted to 45º, with the ball positioned against the chest with both hands. The evaluated could not move their legs and threw the ball with both arms. Three attempts were allowed with 2 minutes of rest between them [18,19], the distances of 2.71 m (0.09) and 2.96 m (0.04) for groups 1 and 2, respectively, were reached in the launches. It was assumed then that the emitter of G2 presented higher performance of explosive force than that of G1.
After 24 hours of the familiarization session, it was followed for the 2nd stage, in which the receivers and emitters performed the warm-up, composed of static stretching, with 15 s duration, with joint range of motion compatible with the sensation of stretching discomfort, actively, for flexion, hyperextension and trunk rotation movements: flexion, extension, adduction, abduction and rotation exercises of the shoulder and pelvic girdle. Then was held a race with self-adjusted pace for 5 min.
Immediately after warm-up, procedures were performed to collect PT. All volunteers remained with the same technical posture of the lower body, known as “sanchin dachi” on Karate Uechi-ryu; where the leg opposite the dominant hand was at the front, knees with a slight flexion, medial left hip rotation and feet distanced to shoulder width. The option for this posture is due to its regular use in the uechi-ryu-style ‘heating’ training of the sample. The upper limbs were positioned on the “seiken ago uchi” guard of this style of Karate (hands closed at the height of the chin, elbows flexed and shoulders in slight flexion), the trunk should remain upright without any apparent rotation (Figure 2).
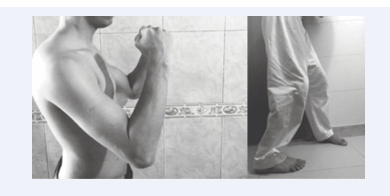
Figure 2: Position for emitters (2A) and receivers (2B).
The techniques were deferred by the emitter in the abdominal region of the volunteer, with the punch technique “seiken zuki” (Figure 3).
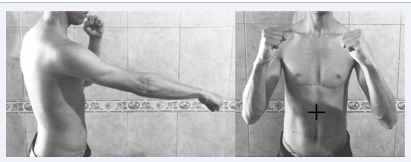
Figure 3: Punch technique and target region.
The kinetics of the technique consisted of a medial rotation of the wrist, elbow extension, slight shoulder rotation and anti-clockwise trunk rotation. The punch technique was always performed at the same site, previously demarcated at the median point between the umbilical scar and the xiphoid process. The cadence between the punches was marked by a portable digital metronome (M50, MEIDEAL) at the rate of 50 bpm. To the sound of each hit a blow was delivered by the IA always with the dominant hand. In the 3rd stage, the punches were throws with a score/intensity 9 in the NRS. When they perceived themselves unable to receive the next blow, given a high perception of pain, the volunteer signaled the withdrawal with his hands and/or verbally. With this, the test was declared closed, and the necessary data were obtained for the analysis of PT. Tolerance as a measure total amount of blows absorbed immediately before withdrawal. The mean duration in the application of the protocol ranged from 6 to 8 minutes of warm-up, and 3 minutes of striking.
Statistical analysis
Categorical variables were presented as relative and/or absolute frequencies. Metric variables were presented as mean (or median when appropriate) and standard deviation (SD) or interquartile intervals. The Shapiro Wilk test was used to verify the normal distribution. The U-Mann Whitney test was used to compare the groups in case of non-Gaussian distribution. Spearman’s test was used to verify possible correlations, assuming r ≤ 0.4 as a weak correlation; r ≤ 0.6, moderate; r ≤ 0.7, strong and r > 0.7 very strong correlation. The p-value was also assumed ≤ 0.05 for statistical differences. SPSS 24 for Windows software was used for data analysis.
RESULTS
Participated in the study twenty-five men karate athletes (32.71 ± 8.22 years, 82.45 ± 9.92 kg, 1.77 ± 0.05 m), with two athletes as emitters and twenty-three others as receivers. The stratifications of the sample mediated by fat percentage (%G) resulted in 13 individuals G1 (%G ≤ 23%) and 10 in the group with %G > 23% (G2). Demographic and body composition data are found in [Table 1].
Pain tolerance for punches was similar (p = 0.36) between the groups (Figure 4).
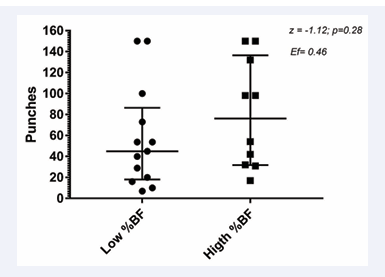
Figure 4: Comparation of the number of punches supported.
The weak correlation between relative fat mass and the number of tolerated striking (Figure 5) was verified.
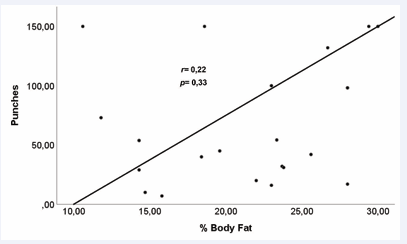
Figure 5: Correlation between the number of tolerated punches and relative fat mass.
DISCUSSION
In contrast to the initial hypothesis, the body fat mass did not influence the pain tolerance to attack techniques in black belts karate athletes. These results do not support the popular understanding between coaches and martial arts athletes. However, the findings presented here do not delimit the concrete relationship between pain tolerability and the body fat mass.
Tabben et al. [20], find that the rating of perceived exertion (RPE) method across the numerical estimation scale is valid for quantifying internal load and intensity in karate training. In the study, the relationship between RPE and physiological parameters such as heart rate and blood lactate concentration was evaluated, and significant correlations were found between RPE and physiological parameters, where the RPE method showed reliability of the same intensity in all training sessions. In this way, we attest to the validity and reliability of the rating of perceived exertion.
The result found in relation to pain tolerance is not only a physiological response to a stimulus, but also depends on parameters related to the psyche of athletes, where previous experiences, emotional state, and psychological control themselves will be largely responsible for identifying and quantifying the painful stimulus received [1,21]. That this, the perception of pain involves the affective-emotional aspect, which directly affects the individual’s ability to tolerate these unpleasant sensations caused by blows delivered to the abdominal region.
Leznicka et al. [22], demonstrated that there is a difference in pain tolerance between athletes of wrestling modalities and non-athletes. Differences in pain tolerance were found in which the athletes had greater tolerance, corroborating the idea that athletes habituated to certain stimulus have higher pain tolerance, as well as in the sample of the present study. On the other hand, we must highlight in our study that both groups are composed of black belt athletes, with great experience in the sport, which in fact, the more trained and skillful the athlete is, the more previous painful experiences he has experienced, which may explain the non-differences between the groups. Additionally, a difference in pain tolerance was observed in athletes of contact sports with different body mass index (r=0.30; p<0.001) [22]. It is suggested then that there be a contribution of the stimulus of contact sports to higher scores of pain tolerance. Possibly, the difference in pain levels in individuals with different body mass index is due to the role of mechanical shock-absorbing of adipose tissue [23]. These results reinforce the hypothesis of the present study since the higher body mass index was positively correlated with pain tolerance. However, in the present study there was no difference between absolute muscle mass (p=0.78) and height (p=0.92) between the groups, so the difference between the total body mass of the volunteers was due to the fat mass. If the absolute results of each group were analyzed, it is noticed that G1 showed lower tolerance to abdominal strokes. Furthermore, Walsh et al. [24], identified positive associations between increased body fat and joint pain. Therefore, the elevated body fat may infer increased risk of worsening joint pain, but in this case, not over skeletal muscle submitted abdominal punches, especially in group 2.
Pain induced by trauma and/or tissue injury activates afferent nerves that carry information to pain processing brain regions [5], in this study we did not collect the pain sensation along the pain tolerability protocol, only the number of blows delivered to the abdominal region. Perhaps, we did not find differences in the number of hits, but possibly one of the groups may have felt more pain and continued in the test. Athletes are individuals who tolerate unpleasant sensations for a longer time; in addition, they have a great perception of self-efficacy that certainly influences the ability to withstand uncomfortable sensations.
There protocol of the pain tolerance used of this study, the measurement of the power of the blow was performed subjectively, not producing absolute values. The distinction of agent issuing blows by group was made respecting the division by category of total body mass. The protocol simulated the moment of reception of the blow at the time of combat. Furthermore, the protocol divided athletes in a similar way to the competitive modality considering their total body mass. However, no similar protocols were found in the literature for comparations. Since there was no difference in relation to absolute muscle mass values, the difference between total body mass was mainly due to fat mass.
Practical Applications
In addition to the possible contribution to the theoretical model that deals with the multifactorial manifestation of pain during the practice of martial arts, these results have practical implications as they refute the common knowledge that athletes with greater fat mass presented larger pain tolerability compared to the leaner. So, such results are relevant to coaches and athletes because with the progressive and adequate training methods it is possible to acquire greater pain tolerance besides of the body compositions differences.
LIMITATIONS
The main limitations of the study would be the subjective control of the intensity of the blows delivered, which limits our discussions about the real vector impact on the abdominal region to verify if the karate athletes were feeling less pain or tolerating the same level of impact throughout. Another limiting factor would be the non-stratification of the psychological profiles of the volunteers since this element can influence pain tolerance.
CONCLUSION
The body fat does not interfere with pain tolerance induced by abdominal punches in experience karate athletes, unlike what is often said in the field of martial arts. Such equality of pain tolerability highlights the importance that trainers must give to the specific experience in Hojo Undo, regardless of the anthropometric profile and body composition of the practitioner.
REFERENCES
2. Leite MP. Dor, sofrimento e luta. Ciencias Sociales y Religión. 2013; 15: 31-47.
3. Clarke M. The Art of Hojo Undo: Power Training for Traditional Karate. 2009.
5. Melzack R, Katz J. Pain. Wiley Interdisciplinary Reviews: Cognitive Sci. 2013; 4: 1-15.
11. Alves Neto O, Costa CM, de C, Siqueira JTT de, Teixeira MJ. Dor: princípios e prática. Artmed. 2009.
17. Pitanga FJG. Testes Medidas e Avaliação em Educação Física. Phorte. 2008; 223.
19. Miller TD. NSCA’s guide to tests and assessments. Human Kinetics. 2012.










































































































































{kind=link}