Point-of-Care Musculoskeletal Ultrasound Evaluation of an Occult Carpal Tunnel Ganglion Cyst Causing Median Neuropathy at the Wrist
- 1. West Virginia University School of Medicine – Eastern Division, Harpers Ferry, USA
Abstract
There are numerous causes of median neuropathy at the wrist. Space occupying lesions within the carpal tunnel represent a minority of median neuropathy causes. We present a case of median neuropathy at the wrist caused by an occult ganglion cyst within the carpal tunnel. Our patient presented with two months of numbness and tingling of the volar thumb and second digit with one week of gradual onset of volar wrist swelling. On point-of-care ultrasound examination, there was a 2.0 x 0.8 x 1.8 cm fluid filled cyst within the carpal tunnel contacting the median nerve. Subsequently, an MRI of the wrist confirmed the size and location of the cyst, and that the cyst was consistent with a ganglion cyst. The patient followed up in the office where an ultrasound guided aspiration and corticosteroid injection of the cyst were performed. The patient followed up at two months and again at 6 months from the initial visit. She had significant improvement and continues to have only minimal symptoms. Our case illustrates the value of point-of-care ultrasound in evaluating masses in the carpal tunnel as a cause of median neuropathy at the wrist. Additionally, ultrasound guided ganglion cyst aspiration can serve as both an immediate and long term solution for median neuropathy caused by a compressing ganglion cyst.
Keywords
Space occupying lesion, Carpal tunnel syndrome, Ganglion cyst, Median neuropathy
CITATION
Sprouse RA, Johnson M (2017) Point-of-Care Musculoskeletal Ultrasound Evaluation of an Occult Carpal Tunnel Ganglion Cyst Causing Median Neuropathy at the Wrist. Ann Sports Med Res 4(6): 1122.
ABBREVIATIONS
CTS: Carpal Tunnel Syndrome; US: Ultrasound; MRI: Magnetic Resonance Imaging
INTRODUCTION
Carpal tunnel syndrome is a common cause of median neuropathy at the wrist affecting between 2.7 to 5.8 % of the adult population [1]. Though CTS is common, the etiology of the condition is often unclear. One overlooked etiology of CTS is space occupying lesions within the carpal tunnel that cause compression to the median nerve. Unless there is obvious swelling or a palpable mass on exam, these space occupying lesions may go undiagnosed as imaging other than radiography is not commonly employed in evaluating CTS. Because the flexor tendons pass through the carpal tunnel, development of a ganglion cyst can occur with irritation to these tendons. A space occupying ganglion cyst can lead to compression of the median nerve and cause CTS.
CASE PRESENTATION
A 49 year old female presented to our clinic for evaluation of two months of gradual onset left volar thumb and index finger numbness and tingling. Mild volar wrist pain and swelling accompanied the numbness and tingling. She denied injury to the wrist, history of wrist osteoarthritis, carpal tunnel syndrome, skin infections, or malignancy. She worked at a packaging facility and performed repetitive activity with her hands. She had attempted ibuprofen and activity modification which had provided little relief. On physical exam, there was a small amount of soft tissue swelling over the volar wrist without skin changes. The soft tissue swelling was slightly tender to palpation but withouta definitive palpable mass. Sensoryexam revealed mild dysesthesias to light touch in the distribution of the median nerve but was otherwise normal. Motor function was intact to the median, ulnar, and radial nerve distribution of the left hand.
Point-of-care ultrasound examination revealed a 2.0 x 0.8 x 1.8 cm fluid filled cyst within the left carpal tunnel that appeared to be contacting the median nerve (Figures 1,2). Further evaluation with MRI confirmed the cyst amidst the flexor tendons within the carpal tunnel. The median nerve was being directly contact by the cyst and the nerve was located to the ulnar aspect of the cyst. Characteristics of the cyst were consistent with a ganglion cyst. Subsequently, the patient underwent an ultrasound guided needle aspiration of 7cc of thick serous fluid and corticosteroid injection of the ganglion cyst (Figure 3). The wrist was wrapped with an elastic compressive dressing and the patient was counseled on activity modification. She followed up in clinic at two months and again at six months from the ultrasound guided procedure. At both visits, the patient had significant reduction
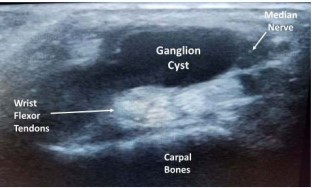
Figure 1: Short axis ultrasound image of ganglion cyst within the carpal tunnel.
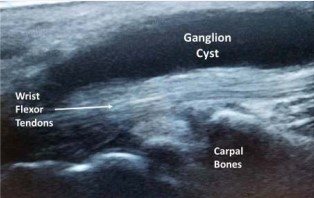
Figure 2: Long axis ultrasound image of ganglion cyst within the carpal tunnel.

Figure 3: Ultrasound guided needle aspiration of ganglion cyst within the carpal tunnel.
in volar wrist swelling. Additionally, she had resolution of her median neuropathy symptoms as evidenced by an improved and now normal sensory exam in the median nerve distribution.
DISCUSSION
Although CTS is a common problem, the etiology of the condition is often unclear. Space occupying lesions of the carpal tunnel are often overlooked as advanced imaging with ultrasound or MRI is not commonly performed in the evaluation of CTS. However, one review found that space occupying lesions in the carpal tunnel caused or contributed to 3% of carpal tunnel syndrome cases [2]. Ganglion cysts, lipomas, tenosynovitis, gout, and uncommon malignancies causing CTS have been reported [2- 5]. CTS commonly presents bilaterally [1,2]. One review of space occupying lesions causing CTS showed that 7 out of 20 unilateral cases of CTS were caused by space occupying lesions as opposed to 89 cases of bilateral CTS where no masses were found on advanced imaging [5]. Some authors have suggested advanced imaging for unilateral CTS where space occupying lesions are more common [4].
Point-of-care ultrasound examination of the carpal tunnel is an effective method for evaluating potential space occupying lesions [6].Additionally, ultrasound guided needle aspiration can be a quick and effective tool for management of carpal tunnel ganglion cysts without the need for surgery. This is especially important when there is evidence of compression of the median nerve. When the characteristics of a space occupying lesion within the carpal tunnel are unclear, MRI can provide further information.










































































































































{kind=link}