Spontaneous Osteonecrosis of the Knee: A review of Past and Present Aspects
- 1. College of Medicine, Howard University, USA
- 2. School of Medicine, University of Virginia, USA
- 3. Department of Orthopaedic Surgery, University of Virginia, USA
Abstract
Spontaneous osteonecrosis of the knee (SONK) is a condition which is known to disproportionately affect women greater than sixty years old. The etiology of SONK is complex without a definitive consensus. The purpose of this paper is to discuss the etiology of SONK on a microscopic and macroscopic level. The patient populations at risk will be highlighted, as SONK can present in athletes and older patients. Staging and imaging studies are critical for understanding the progression of disease and deciding the appropriate treatment option. Nonsurgical and surgical treatment options for SONK will be discussed.
Keywords
Spontaneous osteonecrosis of the knee, Insufficiency fracture, Subchondral collapse, Meniscal extrusion, Athletes
CITATION
Hill WJ, Ruland JR, Diduch DR (2017) Spontaneous Osteonecrosis of the Knee: A review of Past and Present Aspects. Ann Sports Med Res 4(6): 1123.
ABBREVIATIONS
SONK: Spontaneous Osteonecrosis of the Knee; BMI: Body Mass Index
INTRODUCTION
Spontaneous Osteonecrosis of the Knee (SONK) is a stress related insufficiency fracture of the knee that most commonly involves the medial condyle of the femur or medial aspect of the tibial plateau; less frequently it also affects the lateral condyle of the femur [1-4]. Ahlback was the first to describe SONK as a separate pathology from secondary osteonecrosis [2]. In contrast to SONK, Secondary osteonecrosis is true avascular necrosis and the clinical picture consists of patients often less than forty years old with multiple joint involvement. Risk factors for osteonecrosis include alcohol abuse, corticosteroids, high body mass index (BMI), Gaucher’s disease, sickle cell disease, trauma and increased age [5]. SONK manifest in patients in the sixth decade of life or greater with a predilection for women, three times greater frequency than men [1, 3, 5, 6]. The discomfort and pain that occurs in SONK is sudden in nature and causes limitations in functionality of the joint. This pain is markedly severe at night in some patients and persists during rest [1-4, 6]. Symptoms of acute pain due to bone collapse of the insufficiency fracture typically improve with time for healing and optimization of bone health. Residual joint incongruity and osteoarthritis can lead to eventual arthroplasty. This review serves to discuss the etiology, highlight populations at increased risk, underline the importance of staging and imaging modalities in understanding the progression of disease, and discuss appropriate non-surgical and surgical treatment options for stage of disease.
Etiology and Pathophysiology in the text
The Etiology and pathophysiology of SONK has been associated with mechanical, biochemical and traumatic origins. The occurrence of insufficiency stress fractures of the medial femoral condyle and medial tibial plateau has spurred support for the traumatic origin of SONK [7].Though this may play a role in the Pathophysiology of SONK it does not encompass the entire picture. The biochemical process that leads to osteoporosis has been discussed as an alternative etiology. This has been the supported by MRI findings that revealed insufficiency fractures in osteopenic bone [8-10]. Insufficiency fractures are a key finding in SONK and assist in the staging of the condition but a mechanical mechanism may play the largest role. The mechanical etiology of SONK starts with the disruption of the native anatomy of the medial meniscus. Extrusion of the medial meniscus following posterior root tears result in increased stresses across the bone [11-13]. The biomechanical forces that transverse the knee joint are normally buffered by the meniscus. With the meniscus disrupted, the force crossing the knee causes an increase stress on the femur and tibia. Remodeling of bone increases as the stress applied to the bone increases. If the bone cannot strengthen sufficiently to handle the stress then microfractures and bone edema develop [14]. These stress fractures are subchondrally located without the presence of a vascular osteonecrosis [15]. Recent studies have shown meniscal involvement as the predominate associative factor of SONK’s pathogenesis [11-13].
Populations at Risk
The one population at risk that is consistently noted in the literature is older patients greater than sixty years old. Within this cohort women are disproportionately affected three to one [1,3, 5, 6]. Women over sixty years old have a decreased bone mineral density in relation to before menopause [16]. This change increases the chance of fractures, which can manifest as insufficiency fractures of the femur or tibia. Vitamin D deficient patients are another group that needs to be considered at risk for SONK. Within this group includes patients with higher levels of melanin in their skin, such as African Americans, because melanin protects the skin from sunlight which stimulates vitamin D production [17]. The last population that is at increased risk are athletes. This may be the result of repetitive force being applied across the knee joint or underlying meniscal injuries. Repetitive force applied to the knee joint can cause medial femoral condyle defects, particularly in basketball players and runners [18, 19]. Meniscal tear is the most common knee pathology sustained by athletes which would predispose athletes to developing SONK [20]. Also, meniscus tears occur at a greater incidence in athletes than the general population which should rise the clinical suspicion of SONK in athletes and former athletes.
Differential Diagnoses
SONK presents with sudden pain in the affected area of the knee [21]. The acute onset of pain is due to the occurrence of the actual insufficiency fracture and possible bone collapse. During the observation portion of the physical examination the patient may present with an antalgic gait and possible effusion [21]. The knee is not characteristically red in color or warm to touch. During palpation tenderness may be elicited over the affected areas of the medial femoral condyle or tibia [22]. In advanced SONK tenderness of the joint line and crepitus may be found secondary to degenerative changes within the joint.
The differential diagnosis of SONK includes a meniscal tear, osteoarthritis, transient osteoporosis, traumatic bone bruises and fractures, osteochondritis dissecans, tumor infiltration, and pes anserine bursitis. Meniscal tears on physical exam present with joint line tenderness, swelling, and a positive McMurry test [22]. Meniscal tears can be confirmed with an MRI. Osteoarthritis is a condition that is chronic in nature that affects women and men equally as they age. The pain is aching in nature, which will increase with activity and subsides with rest. On plain radiographs tricompartmental involvement is often present rather than just the medial compartment. Osteoarthritis will have secondary radiographic changes of subchondral sclerosis and osteophyte [23]. SONK that remains undiagnosed may go untreated for an extended peiord of time and develop into osteoarthritis [24]. If joint space narrowing is present without these secondary changes, this may represent meniscal extrusion and impending SONK. Transient osteoporosis presents with spontaneous onset of pain. It progresses over several weeks in middle aged men, and also in women in the third trimester of pregnancy. In transient osteoporosis, osteopenia is appreciated that involves the entire condyle [25]. Bone bruises and fractures are trauma associated and will be secondary to a traumatic event. Osteochondritis dissecans consist of the bone separating from its vascular supply resulting in detachment of the cartilage from bone [26]. This involves the lateral portion of the medial femoral condyle most commonly in ten to fifteen year old males. Bone tumors, such as metastasis, may mimic the spontaneous pain of SONK [27]. Pes anserine bursitis originates on the medial aspect of the tibia below the joint line and may radiate toward the joint [28].
Staging and Imaging Findings
Lesions found in SONK are usually located in subchondral bone of the medial femoral condyle and medial tibial plateau. Radiographs and MRIs are the imaging modalities that are used when investigating SONK. The Radiograph views that are recommended are bilateral weight-bearing Posterior anterior (PA), weight bearing 45 degrees flexion PA, non weight bearing lateral and 45 degrees flexed merchant or patella sunrise views. Radiographs can be used to track disease progression. MRI is the confirmatory test and assists in determining the extent of disease that is not appreciated on radiographs [14]. Two key finds on MRI include edema, which indicates stress, and insufficiency fracture with collapse of trabeculae. The staging of SONK can be done by various systems. Aglietti et al. first proposed their system in 1982. According to Aglietti stage I have normal appearing radiographs [2]. Stage II included flattening of the affected weight bearing part of the articular surface of the condyle. Stage III consists of subchondral lesion with radiolucent area of variable size and depth and a surrounding sclerotic halo. Stage IV includes the sclerotic halo with the addition of subchondral bone collapse. Stage V consists of subchondral collapse and secondary degenerative changes. Ficat and Arlet proposed a staging system for osteonecrosis which is modified and used to classify SONK [29]. Stage I lesions are characterized by pain and normal radiographs. Stage II lesions are sclerotic or cystic in nature, with a normal outline of the tibia and femur and without flattening of the joint surface or subchondral fractures. Stage III reveals the characteristic crescent sign which is the result of subchondral collapse. Figure (1) consists of images with subchondral collapse. Stage IV includes joint space narrowing with secondary degenerative changes [30]. Figure (2) below illustrates medial compartment narrowing but without secondary degenerative changes or subchondral collapse. Accurate and early diagnosis of SONK leads to a better prognosis. The use of MRI is the recommended imaging modality as it identifies changes earlier than radiographs and bone scintigraphy [14]. With earlier diagnosis, conservative treatment options have an increased statistical likelihood of being efficacious [31,32]. The imaging findings that have been predictive of poor outcomes, aside from stage, are: lesions greater than 5 cm2 , anatomical varus alignment, lesions affecting greater than 40% of the femoral condyle, and depth greater than 20 mm on MRI [33-39]. These measurements lead to the question of should there be a new staging system in which the size of the lesion is considered.
Treatment Options
The treatment options for patients affected with SONK included conservative, non-surgical, and surgical options. The treatment decided on by the patient and Surgeon takes into account the stage and progression of the disease.
In stages prior to subchondral collapse, conservative treatment has been successful in treating SONK. Conservative treatments include rest, physical therapy, protected weight bearing, and unloader bracing [40]. These options are typically
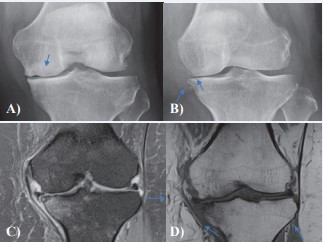
Figure 1: SONK with subchondral collapse. Figure 1A: Radiograph of Subchondral collapse of the medial femoral condyle. Figure 1B: Radiograph Corner fracture of the left medial tibial plateau along with subchondral collapse. Figure 1C: T2 weighted MRI with medial tibial plateau subchondral collapse and fat saturation. Figure 1D: T1 weighted MRI with medial tibial plateau subchondral collapse.
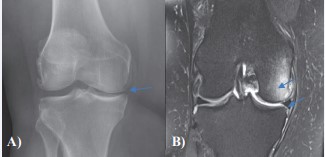
Figure 2: SONK with medial compartment narrowing, absent of secondary signs of osteoarthritis, prior to subchondral collapse. Figure 2A: Radiograph with medial compartment narrowing. Note absence of osteophytes or subchondral sclerosis as would otherwise be expected with this much joint space narrowing. Figure 2B: T2 weighted MRI with medial compartment narrowing and medial meniscus extrusion, fat saturation and extensive bone marrow edema due to ongoing stress reaction of SONK.
done until the bone has healed, which may take as long as six months. Healing of insufficiency fractures takes time, and requires a reduction of applied force on the affected compartment just like any other fracture. The use of a load sensor device is a novel conservative treatment option. It functions by changing the load on the knee through real time biomechanical feedback which results in reduced pain [41]. In athletes that are affected by SONK, hyperbaric chamber therapy has produced promising results [42].
The pharmacological treatment options include oral NSAIDs and narcotics, Vitamin D supplementation, corticosteroid or hyaluronic acid injections, prostacyclin analogue, and bisphosphonates. Oral NSAIDs and narcotics are used to manage painful episodes that SONK produces. In order to maximize bone healing vitamin D levels need to be in the proper range. Vitamin D deficiency and correctable causes of osteopenia and osteoporosis should be addressed to increase fracture healing [43,44]. Corticosteroid or hyaluronic acid injections are options for patients that don’t response to non-pharmacologic conservative treatments. They can reduce inflammation within the joint but will have little effect on bone pain [45]. Prostacyclin analogue, iloprost was mostly studied, increases blood supply to terminal vascular beds [46,47]. It also reduces the amount of free oxygen radicals and leukotrienes in vascular circulation. In studies it provided pain relief and reduced subchondral lesion size, the efficacy is thought to be the result of either returning interosseous pressure to normal or decreasing cytokine and leukotriene local inflammatory reactions [48,49]. The use of bisphosphonates is thought to decrease the resorption of bone by osteoclast as new bone is being formed. This allows for the new bone to be revascularized and limit collapse of bone [50,51].
If a patient progresses to the subchondral collapse stage conservative treatment is still recommended to allow for the fracture to heal. After the fracture has healed the knee will be reevaluated. If pain ultimately still is present operative considerations will be discussed. Surgical options include high tibial osteotomy, subchondroplasty, unicompartmental knee arthroplasty, and total knee arthroplasty. If meniscal root tears are observed, partial meniscectomy should be avoided as it can worsen the condition. Removing more meniscus in the face of meniscal extrusion only increases detrimental forces across the joint [52]. High tibial osteotomy is typically preformed in a young patient. It unloads the medial compartment by correcting alignment of the knee [53]. Subchondroplasty is a newer treatment option for SONK that is not utilized as often as other options but it involves surgically implanting calcium phosphate into trabeculae bone of the lesion [54-56]. Calcium phosphate thereafter crystalizes and stabilizes the fractures. Unicompartmental knee arthroplasty is a viable option for SONK but only when lesions are fully healed and the bone can support the prosthesis without subsidence [57]. This is confirmed by the presence of a normal subchondral sclerosis pattern on radiographs. If there is any doubt about the ability of the bone to support the prosthesis, a total knee arthroplasty is the better option given the broad support [58]. A future treatment option may include the use of stem cell concentrate from bone marrow, as augmentation graft, in conjunction with core decompression.
CONCLUSION
Osteoarthritis and a vascular necrosis of the knee are two differential diagnoses that are often diagnosed when actually SONK is present. With a greater understanding of the pathophysiology and risk factors associated with SONK there may be an increase in incidence of diagnosis. Mechanical factors, specifically meniscus extrusion, may be the precipitating event that leads to SONK. The patient population that represents the traditional clinical picture of SONK are, older women, in the fifth or sixth decade of life. With the understanding that disruption of the native meniscus environment predisposes patients to SONK, athletes and former athletes should also be suspected of potentially presenting with SONK. The current staging classifications are based solely on the character of the lesion without regard to the size. The character of the lesion is important but the size of the lesion may be more specific for disease prognosis.
REFERENCES
22. Meniscus Tears-OrthoInfo - AAOS. 2014.
26. Schenck RC Jr, Goodnight JM. Osteochondritis dissecans. J Bone Joint Surg Am. 1996; 78: 439-456.
31. Jordan RW, Aparajit P, Docker C, Udeshi U, El-Shazly M. The importance of early diagnosis in spontaneous osteonecrosis of the knee - A case series with six year follow-up. Knee. 2016; 23: 702-707.










































































































































{kind=link}