Blunt Abdominal Trauma with Complete Transection of the Main Pancreatic Duct
- 1. Surgical Health Collective, USA
Abstract
A 17 year old male sustained blunt trauma to the epigastrium during a football game. He was transported to a local hospital and evaluated. On admission his blood pressure was 145/96 Pulse – 86 Respiration-16 and oxygen saturation was 98%. His abdomen was soft, non-distended without rebound tenderness. There was no evidence of involuntary guarding. Hemoglobin 13.8 Hematocrit 42 WBC 15,300. INR-1.16 PT 12.6 and PTT 31. Serum lactate was normal at 0.63. His admission amylase was 473 U/L. The admission lipase was 370 U/L. His vital signs remained stable and the initial work up included a CT scan of the abdomen and pelvis. The scan revealed contusion of the body of the pancreas.
Keywords
• Blunt Abdominal Trauma
• Pancreatic Duct
• CT scan
Citation
Walker ML (2023) Blunt Abdominal Trauma with Complete Transection of the Main Pancreatic Duct, South Africa. Arch Emerg Med Crit Care 7(1): 1054.
INTRODUCTION
A 17 year old male sustained blunt trauma to the epigastrium during a football game. He was transported to a local hospital and evaluated. On admission his blood pressure was 145/96 Pulse – 86 Respiration-16 and oxygen saturation was 98%. His abdomen was soft, non-distended without rebound tenderness. There was no evidence of involuntary guarding. Hemoglobin 13.8 Hematocrit 42 WBC 15,300. INR-1.16 PT 12.6 and PTT 31. Serum lactate was normal at 0.63. His admission amylase was 473 U/L. The admission lipase was 370 U/L. His vital signs remained stable and the initial work up included a CT scan of the abdomen and pelvis. The scan revealed contusion of the body of the pancreas. Magnetic resonance cholangiopancreatography (MRCP) was performed but the main pancreatic duct was not visualized. Repeat CT of the abdomen was unchanged. Serum amylase increased to 1549 U/L. Serum lipase increased to 1004 U/L and the patient was taken to the operating room for exploration.
Complete transection of the body of the pancreas was noted. The disrupted main pancreatic duct was visualized (Figure 1).
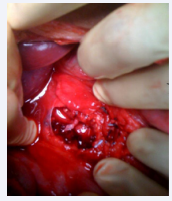
Figure 1: Visualization of the disrupted main pancreatic duct.
The spleen and pancreatic body were mobilized (Figure 2).

Figure 2: Mobilization of the spleen and pancreatic body
The splenic artery and splenic vein were ligated proximal to the area of injury.The pancreatic body and spleen were removed.The main pancreatic duct was sutured with 2-0 silk. The remaining portion of the pancreas was sutured with 2-0 silk sutures as well. 2 Jackson-Pratt drains were placed exiting through separate incisions. The abdomen was closed uneventfully. Post-operatively the amylase level fell to 194 U/L. The patient was able to tolerate a full liquid diet and he was discharged to home with drains in place.
As an outpatient, purulent drainage was cultured from the drains and a heavy growth of Klebsiella pneumoniae (sensitive to flouroquinolones) was documented.Oral levofloxacin was started and the drainage stopped. The patient was tolerating a regular diet and the drains were ultimately removed. A serum glucose level on an outpatient basis was 75 mg. % and a hemoglobin a1c level of 5.9 was noted. The patient continued to progress. He returned to school with advice to avoid contact sports for 3 months.
DISCUSSION
Blunt pancreatic trauma is uncommon overall [1]. The diagnosis may be suspected based on the history of an acute deceleration event with the steering wheel impacting the upper abdomen and compressing the neck of the pancreas against the vertebral column. Bicycle handlebar injuries and blows to the abdomen are the other mechanisms of blunt injury. Aside from epigastric tenderness there may not be much in the way of clinical findings early in the hospital course.
The initial evaluation always centers around the presence of on-going hemorrhage. If hemorrhage is present operative intervention is warranted. If there are no signs of bleeding, evaluation of the pancreas with MRI or repeat CT imaging is recommended. The main issue is the integrity of the main pancreatic duct. If this duct is intact and there is no evidence of transection of a large portion of the pancreas, a non-operative approach is often selected. Grading blunt pancreatic injuries is essential (Table 1).
Table 1: AAST Classification of Pancreatic Injury.
|
Grade 1 |
Minor Contusion or laceration without duct injury |
|
Grade 2 |
Major Contusion or laceration without duct injury or tissue loss |
|
Grade 3 |
Distal transection* or parenchymal injury with duct injury |
|
Grade 4 |
Proximal transection** or parenchymal injury with duct injury |
|
Grade 5 |
Massive disruption of pancreatic head |
East guidelines suggest that Grade 1 and 2 injuries (those without major ductal disruption) are approached non-operatively [2]. With time the area of contusion will heal. In contrast if there is evidence of major ductal disruption (Grade 3 and 4 injuries) operative assessment and therapy is recommended [3]. A distal pancreatectomy (with or without splenectomy) with oversewing of the disrupted duct is usually performed. Stapling the proximal pancreas can be done but a pancreatic fistula remains a risk no matter the approach: stapling vs. hand sewing [4]. In a study reviewing registry data from 18 Level 1 and Level 2 trauma centers, the risk of pancreatic fistula was reduced when the end of the pancreas was managed with staples [5].The DISPACT trial reviewed 352 patients from 21 European hospitals undergoing distal pancreatectomy who were treated with either stapler or a hand-sewn closure. No difference was noted in the pancreatic fistula rate [6]. This question remains unsettled in the blunt trauma setting. In the case presented a low grade infection in the pancreatic bed and a low output pancreatic fistula occurred. The drainage resolved with a short course of oral levafloxacin.
The outcome of patients with blunt pancreatic trauma is based on the presence of vascular injury and other associated injuries [6]. Those patients with vascular injury have the highest mortality and morbidity [6]. Multiple hollow viscus and solid organ injuries will also increase the mortality. CT imaging of the pancreas is useful along with MRI to evaluate ductal structures [7]. If pre-operative imaging reveals ductal disruption there may be a role for ERCP with endocsopic transpapillary drainage and stenting [8]. Even if the CT scan only shows contusion and the status of the main pancreatic duct remains in question amylase and lipase levels may offer additional information. One time amylase levels may not exclude pancreatic injury [9]. Serum lipase may be more helpful and decision tree analysis supports an initial elevation of lipase greater than 306 U/L as suggestive [10]. In the patient presented serial elevations in amylase and lipase prompted operative assessment. Further decision making will be made based on the pathology documented. Major ductal disruption to the left of the superior mesenteric vessels lends itself to distal pancreatectomy with or without splenectomy. If the pancreas is the sole organ injured and the patient is hemodynamically stable, distal pancreatectomy with splenic preservation can be performed [11]. If the injury is to the right of the superior mesenteric vessels ductal ligation might be a consideration although data regarding this is lacking [12]. In both instances, drainage of the pancreatic bed is essential. For devastating injuries to the head of the pancreas, control of hemorrhage is primary and a damage control approach may be required [12]. These patients should be monitored in the intensive care unit post-operatively as they will often require ongoing resuscitation.
If a damage control approach is selected, planned reoperation once coagulopathy has resolved and hemodynamics are stabilized is mandated [13,14]. Pancreatoduodenectomy is a huge undertaking in an acutely ill trauma patient and is rarely needed in the setting of blunt injury.
Pancreatic injuries detected during abdominal exploration should be drained. Drains should remain until drainage has resolved.
The patient presented maintained a normal glucose with a one-time mild elevation of hemoglobin a1c. Diabetes can occur over the long-term with limited islets because of the distal resection.
In summary, blunt trauma to the pancreas must be considered based on mechanism of injury. If detected early and main pancreatic ductal injury is suspected, operative intervention is warranted. Grading of the injury is essential. Non-operative therapy for Grade 1 or 2 injuries is recommended. Operative management for major ductal disruption is considered standard therapy. ERCP and stenting of major ductal injury in the setting of blunt trauma is being used more often in the current era. If pancreatectomy is necessary, active drains should be placed in the pancreatic bed. Careful monitoring for infection in the post operative period is indicated. Using these principles, excellent outcomes should be achieved.
REFERENCES
- Lin BC, Chen RJ, Hwang TL, Lessons learned from isolated blunt major pancreatic injury: Surgical Experience in One trauma Center Injury. 2019; 50: 1522-1528.
- Ho VP, Patel NJ, Bokhari F, Madbak FG, Hambley JE, Yon JR, et.al Management of Adult Pancreatic Injuries: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma and Acute Care Surg. 2017; 82: 185-199.
- Biffl WL, Moore EE, Croce M, Davis JW, Coimbra R, Karmy Jones R, et.al Western Trauma Association Critical Decisions in Trauma: Management of pancreatic injuries J Trauma and Acute Care Surg. 2013; 75: 941-946.
- Probst P, Huttner F, Klaiber U, Knebel P, Ulrich A, Buchler MW, et al Stapler versuss scalpel resection followed by hand-sewn closure of the pancreatic remnant for distal pancreatectomy Cochrane Database Syst Rev. 2015; 6: CD008688
- Byrge N, Heilbrun M, Winkler N, Sommers D, Evans H, Cattin LM, et al. An AAST-MITC analysis of pancreatic trauma: Staple or sew? Resect or drain? J Trauma Acute Care Surg. 2018; 85: 435-443.
- Diener M, Sieler C, Rossion I, Kleeff J, Glanemann M, Butturini G, et al. Efficacy of Stapler versus hand-sewn closure after distal pancreatectomy (DISPACT): a randomised controlled multicentre trial. Lancet. 2011: 377: 1514-1522.
- Ull C, Bensch S, Armin T, Swol J. Blunt Pancreatic Injury in Major Traum: Decision-Making between non-operative and operative treatment. Case Rep Surg. 2018: 6197261
- Chen Y, Jiang Y, Qian W, Yu Q, Dong Y, Zhyu H, et al. Endoscopic transpapillary drainage in disconnected pancreatic duct syndrome after acute pancreatitis and trauma: Long term Outcomes in 31 patients BMC Gastroenterol. 2019; 19: 54.
- Donkin IE, Jones R, Aldous C, Clark DL. A prospective evaluation of the predictive value of serum amylase levels in the assessment of patients with blunt abdominal trauma. S Afr J Surg. 2015; 53.
- Rau CS, Wu SC, Chien PC Kuo PJ. Identification of Pancreatic Injury in Patients with Elevated Amylase or Lipase level Using a Decision Tree Classifier: A Cross- Sectional Retrospective Analysis in a Level I Trauma Center. International Journal of environmental Research and Public Health 2018, 15. 277 Licensee MDPI Creative Commons Attribution (CC BY) license(http:..creativecommons. org/licenses/by/4.0/)
- Pachter HL, Hofstetter Sr, Liang HG, Hoballah J. Traumatic injuries to the pancreas: the role of distal pancreatectomy with splenic preservation. J Trauma 1989; 29: 1352-1355.
- Ordonez C, Parra M, Millan M, Caicedo Y, Padilla N, Minan Arana F, et al. Pancreatic damage control: the pancreas is simple don’t complicate it Colmb Med(Cali). 2020; 51: 4054361.
- Krige J, Kotze UK, Setshedi M, Nicol AJ, Navsaria P. Management of pancreatic injuries during damage control surgery: an observational outcomes analysis of 79 patients treated at an academic Level 1 trauma center. European J Trauma Emergency Surg. 2017; 43: 411-420.
- Duschesne JC, Kimonis K, Marr AB, Rennie KV, Wahl G, Wells JE, et al. Damage Control Resuscitation in Combination with Damage Control Laparotomy: A Survival Advantage. J Trauma. 2010; 69: 46-52.









































































































































{kind=link}