MEG Study with Pico-Tesla External TMS on Children with Dystonia
- 1. Department of Medical Physics, Democritus University of Thrace, Greece
- 2. Department of Electrical Engineering, Democritus University of Thrace, Greece
Abstract
Magnetoencephalographic (MEG) recordings were obtained in children with dystonia, in order to look for possible effects using external pico-Tesla transcranial magnetic stimulation (pT-TMS). We used a whole-head 122 channel MEG system. The study was consisted of 8 children with dystonia (7 male, 1 female) ranging from 9-12 years of age (mean: 10 ± 1.3). The pT-TMS was applied to the above children with proper field characteristics (magnetic field amplitude: (1-7.5pT) and frequency: the alpha-rhythm of each child 8-13Hz).We have found a significant effect of an increase in the 2-7Hz frequencies range toward the patients’ alpha-rhythm which is ranged from 8-13Hz and were above the baseline frequencies. The children were not complained using the pT-TMS device and the results were statistically significant at 5 out of 8 (62.5%) children with dystonia. This method of the pT-TMS has some prospective effects to be considered as a non invasive safe and efficient modality in managing the symptoms in children with dystonia.
Keywords
• MEG
• Children with dystonia
• pT-TMS
• Brain frequencies
Citation
Anninos P, Adamopoulos A, Kotinisor A, Tsagas N (2017) MEG Study with Pico-Tesla External TMS on Children with Dystonia. Arch Paediatr Dev Pathol 1(1): 1004.
INTRODUCTION
Transcranial magnetic stimulation (TMS) is a non-invasive technique which has a variety of diagnostic and therapeutic uses in clinical conditions [1-3]. The signal which we can get with the Biomagnetic measurements which were performed using a wholehead 122-channel MEG device is called Magnetoencephalogram (MEG) and is regarded as the most efficient method for recording brain activity in real time. It has unique sensitivity to CNS disorders and normal brain functions and also is a wellestablished non-invasive method, for investigating human brain activity with whole head neurophysiological measurements. The MEG offers functional mapping information and measurement of brain activity in real time, unlike CT, MRI and fMRI which only provide structural, anatomical and metabolic information. In addition with the MEG the brain is seen in “action” rather than viewed as still image. Furthermore, the MEG has the ability to resolve msec temporal activity which is associated with the information processing which is the main task of the human brain. Finally, the MEG measures weak magnetic fields which are generated at the scalp surface by the underlying electrical activity in the brain and it is very significant for diagnostic purposes. Furthermore, TMS is mainly useful to establish with MEG map causal brain-behavior relations in motor and non-motor cortical areas. Shelley and Trimble [4], suggested that MEG, data fusion models, TMS, evoked potentials, intracranial electrophysiology, and EEG complemented by fMRI and PET would definitely help in further understanding the broader connection between brain and motor behavior.
Albanese et al., [5] in a review article reported that the use of repetitive TMS (rTMS) has been assumed to reduce abnormal cortical excitability, thus improving dystonia. Recent studies reported clinical, neurophysiologic, and imaging improvements after rTMS in patients with focal hand dystonia, axial dystonia or cervical dystonia [6-8]. Additionally, it was found that transcranial direct current stimulation of the motor cortex may improve hand motor control in musicians or children with dystonia [9,10]
Anninos et al. [11], suggested that pico-Tesla (pT) (1pT= 10-12 T) external transcranial magnetic stimulation (pT-TMS) to patients has some quantifiable benefits. Using external weak pT-TMS they were able successfully to attenuate seizure activity in a cohort of over 100 patients with various forms of epilepsy. Specifically, using an electronic device [13], they were able to increase frequencies of the (2-7Hz) posterior dominant rhythms of the brain activity towards frequencies of less than or equal to those frequencies of the alpha frequency range (8- 13Hz) of each patient [13-23]. One possible electrophysiological explanation for the efficacy of pT-TMS has been provided by the proposed “Neural Net Model” [19] that suggests that pT-TMS causes a temporally modulated neuronal inhibition in regions exhibiting abnormal activity in the frequency range of 2-7Hz. This hypothesis is in accordance with data presented by other investigators [24-26].
There are no studies in the literature reported the effects of pT- TMS on children with dystonia using MEG. Thus, the aim of this research was to identify any change in the state between brain and motor behavior in children with dystonia involving involuntary movements, muscle contractions and other movements disorders like twisting body movements, tremor and unusual or awkward postures.
METHODS AND RESULTS
Diamagnetic measurements were performed using a whole-head 122-channel MEG device (Neuromag-122, Neuromag Ltd. Helsinki, Finland). Recordings were taken in an electromagnetically shielded room. The spontaneous MEG recordings were taken with sampling frequency rate of 256Hz and associated Nyquist frequency of 128Hz. The MEG signal was filtered with cut-off frequencies at 0.3 and 40Hz.
All the children with dystonia were 8 (7 male, 1 female) ranging from 9-12 years of age (mean: 10 ± 1.3) and they were without medications during their examinations. The research was approved by our University Research Committee (project number: 80347). In all patients informed consent for the methodology and the aim of the study was obtained prior to the procedure. All children were referred to our lab by practicing neurologists. In this study we set out to show the effect of pTTMS in children with dystonia using the MEG recordings before and after pT-TMS. In our study we haven’t included healthy subjects as controls because this research was already published by Troebinger et al.[27].
All the children with dystonia were at rest with their eyes closed in order to avoid artifacts and to enhance alpha rhythm during MEG recordings. The head was stabilized within the whole-head 122-channel MEG helmet with plastic patches during MEG recordings. Four indicator coils were attached to the head of each patient in order to determine the exact position of the head with respect to the MEG device sensors. The exact positions of the coils were determined using a three dimensional head position indicator (HPI) digitizer. All MEG data tracings were visually inspected carefully off-line for movement artifacts and periods contaminated with movement artifacts were cut off. The time taken for each recording was 2min in order to ensure alertness for each subject. With this in mind, the time frame of our clinical investigations was in the following way:
1st day: MEG measurements in our lab. Application of pT-TMS and MEG recordings afterwards.
2nd day: The MEG spectrum was almost normal in the majority of the children with absence most of the abnormal posterior frequencies at (2-7Hz). Examination by two clinicians, confirmed our findings of normalization of our MEG recordings and patient symptoms
10th day: MEG recordings and evaluation by the same clinicians. Most of the children reported a progressive deterioration of their pretreatment status.
To confirm that the responses to pT-TMS treatment were reproducible we advised the relatives of all patients to apply the pT-TMS electronic device treatment nightly at home (23:00pm).
The pT-TMS electronic device is a modified helmet containing up to 122 coils which are arranged in 5 array groups, so as to cover the 7 brain regions (frontal, vertex, right and left temporal, right and left parietal and occipital) for each subject. It is designed to create pT-TMS range modulations of magnetic flux (intensity: 1-7.5 pT), in the alpha frequency range (8-13Hz) of every child with dystonia. The pT-TMS device was configured for each patient to generate a square wave activity as is stated in [11,12]. A software program was developed in our lab in order to detect the amplitude of the primary dominant frequency of the power spectra of the MEG recordings obtained from each patient with dystonia and channel after the application of Fast Fourier Transform (FFT). Then we looked at (alpha rhythm: 8-13Hz) for calibration of the electronic device and for frequencies at (2-7Hz) for the analysis.
In Table (1) shows the brain regions and the corresponding channels in each brain region. In Table (2) shows the symptoms in each of the children with dystonia evaluated by two clinicians according to the American Classification of the Unified Dystonia Rating Scale, (UDRS) [28], one month after daily pT-TMS treatment at home, following the instructions given to the relatives of all patients .It was observed an improvement in the dystonia symptoms at 5 out of 8 children with dystonia (62.5%). Figure (1)
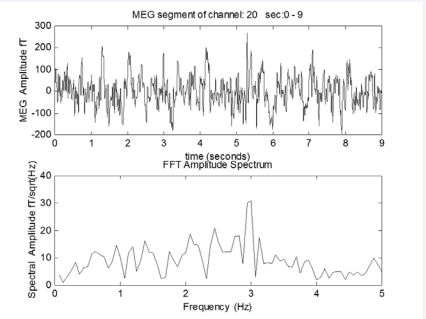
Figure 1
A) The MEG obtained from a dystonia child
B) After the application of FFT on the above MEG we get primary dominant frequency of 3Hz.
shows the MEG record obtained from a child with dystonia and the application of FFT on the above MEG record which gives the primary dominant frequency at 3Hz.
DISCUSSION
In our research we have attempted to influence the patients with dystonia with the pT-TMS electronic device(13).The coils of the device were constructed to emit back to the brain of the patients magnetic fields with proper field characteristics( magnetic field amplitude: (1-7.5pT) and frequency: the alpharhythm of each child 8-13Hz). This resulted to decrease of the maximal magnetic power emitted from these areas and an attenuation of the dystonia activity observed by the clinicians. As a final point to confirm that the responses to pT-TMS were reproducible we have advised the relatives [11], of all children with dystonia to apply the pT-TMS treatment nightly at home (23:00 pm).
After one month of pT-TMS treatment at home all the children with dystonia were evaluated again with MEG recordings and interview by the same clinicians and their benefit from this treatment it is shown in Table (2).
The mechanism by which the application of the pT-TMS has some beneficial effects in the children with dystonia is unidentified. Although, one possible explanation is that these magnetic fields (pT-TMS) have been shown to influence the activity of the pineal gland (PG) which regulates the endogenous opioid functions [29], and the dopaminergic modulation [30], GABA [31]. Moreover, the PG is a regulator of our immune system through the action on the thymus gland generating the infection fighting T-cells which are needed to neutralize foreign invaders such as viruses and bacteria. If the thymus gland shrinks with the age or due to other disorders its ability to generate T-cells is sapping.
In conclusion, this method of the pT-TMS has some possible effects to be considered as a non invasive safe and efficacious modality in managing the symptoms of children with dystonia where we have 62.5% effect of using the pT-TMS. Nevertheless further investigation with more patients are required in order to estimate the possible effect of pT-TMS and its significant contribution for managing the symptoms of children with dystonia.
Table 1: It is shown the brain regions and the corresponding channels.
| Brain Regions | Channels |
| Frontal | 17-42 |
| Occipital | 75-86,91-96 ,101-110 |
| Vertex | 13-16,49-54,61-66,73,74,89,90,99,100 , 117-122 |
| Right Temporal | 1-14 , 111-120 |
| Right Parietal | 5-6,11-16,97-100,109,110 , 115-122 |
| Left Temporal | 43-50 ,55-62,67-74 |
| Left Parietal | 47-52,59-64,71-74,79,80,87-90 |
Table 2: The symptoms of the 8 dystonia children before and after pT-TMS as were evaluated by interview by clinicians according to the American Classification of the Unified Dystonia Rating Scale, (UDRS), one month after daily pT-TMS treatment at home (F:Female; M:Male).
| Patient Code | Age | Sex | Symptoms before pT-TMS | Symptoms after pT-TMS |
| 1 | 9 | F | Focal dystonia where one part of the body is effected(UDRS:3) | She has a good effect (UDRS:0) |
| 2 | 9 | M | Generaliged dystonia where both legs and other regions of the body are effected (UDRS:3) | No effect. (UDRS:3) |
| 3 | 9 | M | Generalized dystonia where both legs and other regions of the body are effected (UDRS:3) | He was feeling better (UDRS: 0) |
| 4 | 9 | M | Focal dystonia where one part of the body is effected(UDRS:3) | He was feeling better (UDRS: 0) |
| 5 | 10 | M | Focal dystonia where one part of the body is effected(UDRS:3) | No effect(UDRS:3) |
| 6 | 10 | M | Multifocal dystonia where at least two regions of the body that are not connected to each other are affected as for example in this case one arm on one side as well as one leg of the other side of the body (UDRS:3) | He has effect in both sides of his body (UDRS: 0) |
| 7 | 12 | M | Segmental dystonia where two or more regions of the body are affected and the regions somehow are connected to each other as for example neck and shoulder (UDRS:3) | No effect(UDRS:3) |
| 8 | 12 | M | Focal dystonia where one part of the body is effected(UDRS:3) | Very good effect(UDRS:0) |
SOURCE OF FUNDING
Funding for this work was provided by a collaboration of GGET (General Secretariat of Research and Technology, GR) and ERGO AEBE, INC, GR under the research program titled “Foundation of a Laboratories Network and purchase of a Multichannel Biomagnetometer SQUID (Superconducting Quantum Interference Device), in order to develop an expert system for automatic acquisition, analysis, evaluation and exploitation of MEG signals that are emitted from different organs of the human body” (Grant Number: 80623).









































































































































