Diaphragmatic Hernia-Rare Case Scenarios
- 1. Department of Pediatrics, Government Medical College, India
Abstract
Diaphragm is the partition between thoracic and abdominal cavities. Embryologically it develops primarily from septum transversum. Some parts of diaphragm has its origin from pleuraeritoneal membrane, mesoderm of the posterior body wall, ventral and dorsal mesenteries of esophagus.
Hence, defect in fusion of them leading to congenital anomalies are also common. Abdominal contents may pass through these defects causing diverse types of diaphragmatic hernia. Such hernias are more common on left side than right.
Classification of Diaphragmatic Hernia (DH) according to anatomical location
1) Posterolateral: due to failure of pleura-peritoneal canal to close (commonest type)
2) Posterior: due to failure of development of the crura
3) Retrosternal: due to an anomalous large gap between the sterna and costal parts of the muscle
4) Central: through the dome of the diaphragm.
Rarely the diaphragmatic muscle may be thin and aponeurotic, may bulge upwards in to the thorax. The bulging may be unilateral or may be confined to a small area. This condition is called congenital eventration of the diaphragm. Usually these congenital anomalies of diaphragm are manifested at birth or in infancy. When they present in later age group, they cause wide variety of symptoms, making the diagnosis difficult. Here we present four different cases of diaphragmatic anomalies which had confusing clinical presentation. All cases were managed successfully.
Keywords
• Diaphragmatic hernia
• Pleura-eritoneal membrane
• Congenital anomalies
Citation
Ananda Kesavan TM, Thuruthiyath N, Balakrishnan I (2017) Diaphragmatic Hernia-Rare Case Scenarios. Arch Paediatr Dev Pathol 1(3): 1012.
CASE 1
A 4-year-old girl was admitted with history recurrent respiratory tract infections. She had already taken 3 courses of parenteral antibiotics without showing improvement. She was fully immunized and had no history of contact with tuberculosis. On examination, she was a well thriving child with normal weight and height, not looking toxic or dyspneic. Respiratory system examination showed decreased air entry on left lower lung zones. She was investigated. All her routine examinations were normal. Diagnostic tests for tuberculosis and HIV were also negative. Her chest X-ray showed non homogeneous opacity on left side with shifting of mediastinum to right (Figure 1). An MRI chest showed diaphragmatic hernia on left side –stomach, intestine and spleen herniating into the thorax with displacement of heart (Figure 2). She underwent surgery and recovered and is doing well on follow up (Figure 3).
CASE 2
A 4yr old girl who visited our outpatient department gave history of fever and cough. Mother also complained of coughing while eating, noticed since a week. No other remarkable history except for several upper respiratory infections in the past. She was fully immunized. On examination: her vitals were normal. General and systemic examinations were normal. Since mother had given a history suspicious of choking, an X-ray of chest was taken (Figure 4). Chest X-ray showed a cyst like shadow on lower chest region on right side. There was no evidence of fluid in the cyst, but showed some irregular opacity. An USG of abdomen and thorax performed showed suspected bowel loops inside the chest. A barium study, as advised by the pediatric surgeons, was done which revealed the diagnosis (Figure 5). It showed loops of intestine (large) herniating into thorax-suggestive of Morgagni – Larrey hernia. Child underwent surgery, also with a confirmation of diagnosis and was managed well.
CASE 3
A 15-month-old boy was admitted with fever, cough and breathlessness of 6 days duration. Mother gave a history of aspiration while feeding and hospital admissions three times in the past, for suspected aspiration pneumonia. Mother also had given history of severe cough while feeding, on several occasions in the past. He was fully immunized, His weight was only 7.2 kg, and otherwise an active child. All his developmental mile stones were normal. His system examination including lower cranial nerves were normal. All routine investigations including screening for HIV and tests for tuberculosis were unremarkable. His chest X-ray taken outside was reported normal (Figure 6). On careful examination, we suspected some abnormal shadow behind heart and so further investigated. USG abdomen showed abnormal bowel loops on the side of lower end of esophagus. Later a barium swallow study showed sliding hiatus hernia (Figure 7). Child underwent surgery. On follow up he was asymptomatic and gained 2kg weight in a span of 8 months.
CASE 4
A 4-yearboy was referred to us with retro-sternal chest pain of 3month duration, which was aggravated following food intake and in lying down position. He was treated with anti reflux medications and PPI without much relief. All his routine investigations were normal. X-ray chest showed large cavity on left side with air fluid level (Figure 8). Mediastinum was shifted to right. A history of attempted thoracocentesis in a local hospital suspecting fluid in the chest was also given. Since lung shadow was not visualized on left side, eventration was suspected. A Ryle’s tube was inserted and contents were aspirated (Figure 9). Child underwent surgery, and presently doing well.
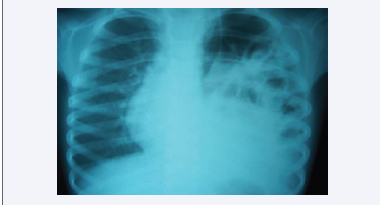
Figure 1 X- ray chest showing non- homogeneous opacity on left side. Also note the shifting of mediastinum to right.
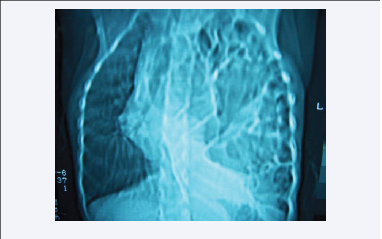
Figure 2 MRI chest showing intestines and spleen inside left thoracic cavity.
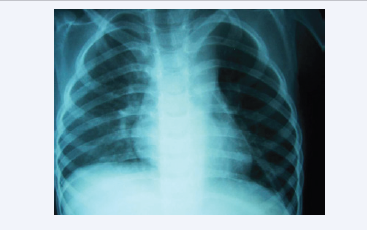
Figure 3 Post operative film of case in Figure 1 and 2. Lung is fully expanded (drainage tube in situ).
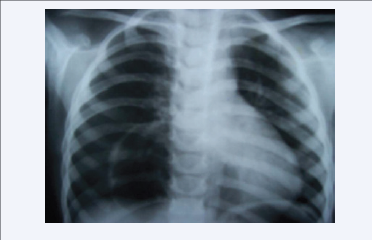
Figure 4 CXR showing round cystic mass right lower lung field adjacent to right heart border.
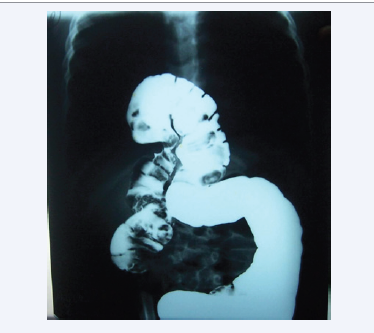
Figure 5 Barium study showing loops of intestine herniating in to thorax- Morgagni hernia.

Figure 6 CXR of a child with recurrent aspiration. Suspected air shadow behind the heart.
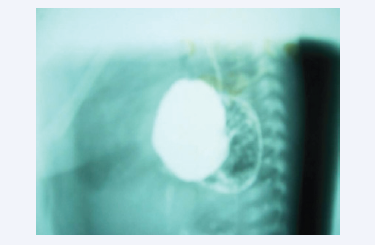
Figure 7 Barium swallow study (lateral view) showing sliding hiatus hernia.
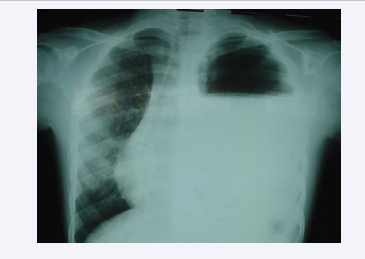
Figure 8 X-ray chest showing large cavity on left side with air fluid level.
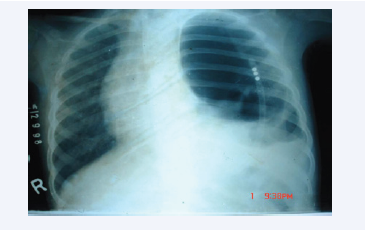
Figure 9 Same child in Figure 9, after aspiration of stomach contents- Eventration of diaphragm
DISCUSSION
Diaphragmatic Hernia (DH) is a rare congenital anomaly of diaphragm [1]. The incidence is I in 2-5000 live births with a greater incidence in still birth and abortions [2]. The commonest one is Bochdalek hernia (75-85%) which usually presents at birth. If manifesting at birth, it is associated with high mortality (up to 50%) owing to the mechanical effect of contents of hernia and due to associated pulmonary hypoplasia [3]. Other associated anomalies will be seen in 10-20% of DH. Along with respiratory distress, they present with clinical features like scaphoid abdomen, mediastinal shift and bowel sounds in the chest, at birth. 50-80% of DH is detected by antenatal ultrasound scanning [4]. Improved surgical techniques and newer ventilator support (ECMO), has improved the outcome of the disease. Very rarely DH may present in older children (and even in adults). They present differently - may remain asymptomatic or to recurrent respiratory tract infection as described in above cases. Diagnosis may quite be difficult if they present at a later age, though prognosis is good [5]. The DH who present after 24 hours of birth have a 100% chance of survival [4].
Morgagni hernia is still a rare (2%) type of DH and is due to an anterior defect in the diaphragm. It is characterized by herniation of contents through the foramina of Morgagni which are located immediately adjacent and posterior to the xiphoid process of the sternum. Majority of them are detected accidently while taking X-ray for some other purpose. Rarely may they get strangulated. Hiatus hernia can be asymptomatic or can present with recurrent respiratory tract infections, regurgitation of feeds or failure to thrive. Since clinical features are non-specific, a high index of suspicion is needed. A chest X-ray and upper GI series are essential to reach the diagnosis. Endoscopy maybe needed occasionally.
Eventration of the diaphragm is an abnormal elevation of the dome of diaphragm in which all or a part of the diaphragm is largely composed of fibrous tissue. Clinical manifestations range from asymptomatic to life threatening respiratory distress. It is a rare disorder with 3 cases affecting every 10,000 neonates [6]. Male and left sided predominance is noted. Associated anomalies may be present in a considerable number of cases, the commonest being the cardiac and chromosomal, which have a strong bearing on the outcome of treatment.
CONCLUSIONS
The cases reported in our study are delayed presentations of DH-Bochdalek hernia, Morgagni hernia and hiatus hernia respectively. All of them presented beyond infancy and hence the clinical features are atypical. When a case of DH will present in later age group, a high index of suspicion is needed. All of them were diagnosed using conventional radiograph (and barium studies) and later confirmed with MRI. In general, plain X-ray remains to the primary radiological investigation of choice. The treatment of choice is surgery. All of them underwent surgical correction and recovered well.
The child with diaphragmatic eventration also presented in older age group, as hydropneumothorax and even performed needle aspiration. Diagnosis was confirmed by a simple procedure like Ryle’s tube aspiration and he underwent surgical repair. The variable clinical features of CDH presenting beyond the neonatal period may result in clinical and radiological misdiagnosis.









































































































































