Progressive Music Activation Enhances Selective Attention in Healthy Older Adults and Alzheimer
- 1. Neuroscience Institute of Castile and Leon, University of Salamanca, Spain
- 2. Department of Psychology, University of Salamanca, Spain
Abstract
Objectives: This study aims to demonstrate the effectiveness of progressive music activation to improve selective attention in patients diagnosed with Alzheimer’s disease (AD) and healthy older adults.
Methods: 58 residents of senior centers or Alzheimer’s units aged over sixty-five participated in the study. Treatment group allocation was performed with permuted block randomization. Experimental group (Age, x? = 80,35; MMSE, x? = 21,14) underwent 12 thirty-minute progressive music activation group sessions, conducted twice a week for six consecutive weeks. The rest of subjects (Age, x? = 79,41; MMSE, x? = 21,55) participated in a conversation group activity. To measure the efficacy of the therapy, we evaluated the general cognitive state of the participants by MMSE and a pre-post evaluation of their attention capacity applying an adapted version of the visual search task [1].
Results: We confirmed that the attention span of visual search improved significantly in persons who underwent the progressive music activation intervention
Conclusion: Progressive music activation could be considered as an enhancer of selective attention in patients with Alzheimer’s disease and in healthy older persons (HOA).
Keywords
- Alzheimer’s disease (AD)
- Progressive music activation
- Selective attention
- Visual search
- Cognition
CITATION
Carcavilla N, Meilán JJG, Carro J, Ivanova O, Arana JM (2017) Progressive Music Activation Enhances Selective Attention in Healthy Older Adults and Alzheimer’s Disease Patients. JSM Alzheimer’s Dis Related Dementia 4(1): 1034.
ABBREVIATIONS
MCI: Mild Cognitive Impairment; AD: Alzheimer’s Disease; HOA: Healthy Older Adults; NPS: Non-Pathological Senescence
INTRODUCTION
Listening to music activates auditory cortex and a widespread bilateral network of brain regions, which include basal ganglia, cerebellum, dorsal premotor cortex and supplementary motor area [2], areas related to attention, semantic processing, memory, motor functions, and emotional processing [3]. It is probable that the integrating capacity of music provides it with a better ability to favour neuronal plasticity in healthy elderly and in AD patients. So, this role of music could be exploited for developing new therapies for improving cognitive abilities.
Music-based therapeutic interventions were already used in order to improve behavioural and psychological symptoms of dementia and to adjust both cognitive impairments and emotional factors [4-8]. Thaut [9] stated that listening to music could take over the role of activation, guidance and adjustment of attention
For patients after stroke, Särkämö et al. [10], found that recovery in the domains of focused and sustained attention improved significantly more in a music-listening group than in control groups. This domain seems to be implicated in Alzheimer’s disease as well [11]. Whereas sustained attention is apparently preserved in persons with Alzheimer’s, other types of attention - like divided attention or selective attention – seem to be rather more vulnerable to impairment during the first stages of dementia, that is, when people are unable to concentrate and are dominated by irrelevant surrounding information [12]. Apparently, the most impaired tasks are those which depend on the spatial shifting of attention from one stimulus to another [13].
The ability to pay selective attention to relevant information without being distracted by irrelevant stimuli is a process, which deteriorates with age (for a review, see [14]). An age-related decline is frequently evident in the overall efficacy of visual search performance, but the selective allocation of attention to task-relevant information, expressed as changes in performance associated with target-location and target-identity cues, is in many respects constant as a function of age [15]. So, in healthy ageing, attention impairments apply in the same way, although they happen much more rarely [16].
Attention is responsible for the proper functioning of other mental processes, like memory, executive processes and coping with difficulties in daily life activities. Therefore, it is necessary to work to maintain attentional processes as well as possible. It has been repeatedly suggested that fast-tempo music increases the rate of breathing, heart rate and blood pressure, whereas slow music, like sonnets or adagios, produces the opposite effect [17]. These observations intended to point at the direct effect that classical music makes over activation and inhibition levels of attention in humans. The music of many composers effectively improves the quality of life, may enhance health and even probably extend the life, which is particularly true for music by Bach, Mozart or Italian composers [18].
So, listening to such classical composers for a few minutes could boost the conscious perception by increasing the activation level or arousal triggered by changes in electrodermic, cardiovascular and respiratory activities [19-21]. In addition, the recovery of vascular and respiratory functions, which improve the levels of cortisol produced by stressful situations, will be regulated [22-24]. Thanks to this evidence, it is possible to assert that music – classical music mainly – has an analgesic effect in reducing anxiety and refocusing attention out of the negative experience [25-29].
The objective of this research is to study the influence of progressive music activation on the capacity of selective attention in the elderly with non-pathological senescence (NPS) and patients with AD. The effects of the intervention will be notable in persons with NPS and in patients with AD as well. We hypothesize that progressive music activation will improve the performance on selective attention task in the elderly with and without dementia when compared with the performance on the same task in people who participated in conversational group event.
MATERIALS AND METHODS
Participants
A total of 80 persons from three retirement homes in Salamanca (Spain) were contacted for participation. 67 persons accepted to participate, but only 58 fulfilled our inclusion criteria. The inclusion criteria were: to be over 65 years old; to have been for at least three month in a retirement home; to have obtained over 11 scores in MMSE, and to preserve communicative ability in order to be able to maintain a coherent conversation. Participants were excluded if they had any history of clinically significant depression or uncorrected visual or hearing problems. The sample (n=58) was randomized. All subjects were people over sixty-five years old who either live in senior centers or Alzheimer’s units. Patients with AD met the criteria set forth by NINCDS-ADRDA, and they were recruited from the clinical population of the State Reference Centre for Alzheimer’s, as well as from two senior centers in the town of Salamanca (Spain). Healthy controls were recruited from the same two residences, thus sharing with AD patients the characteristic of being institutionalized subjects from senior centers. HOA were defined as people who show no cognitive impairment on a standard battery of neuropsychological tests, with MMSE scoring ≤ 23 and SET-TEST scoring ≤ 27 (Table 1), and contrast these results with the clinical history provided by the senior centers. Patients who met the inclusion criteria were informed about the study, including its objectives, duration and data use. There were 34 patients with a clinical diagnosis of AD and 24 HOA, all of them were randomly assigned to either the experimental group (18 patients with AD and 11 HOA; a total of 29 subjects received the intervention and all of them finished the study) or control group (16 patients with AD and 13 HOA) by permuted block randomization (Figure 1). It was stressed on that their participation in the study would not interfere with their medical treatment, and that no invasive techniques were going to be used. Informed signed consents were obtained from either the participants or their legal guardians. All information and data obtained from the subjects is confidential and will only be used for legitimate research purposes. The ethical committee of the State Reference Centre for Alzheimer’s passed the study before it was carried out.
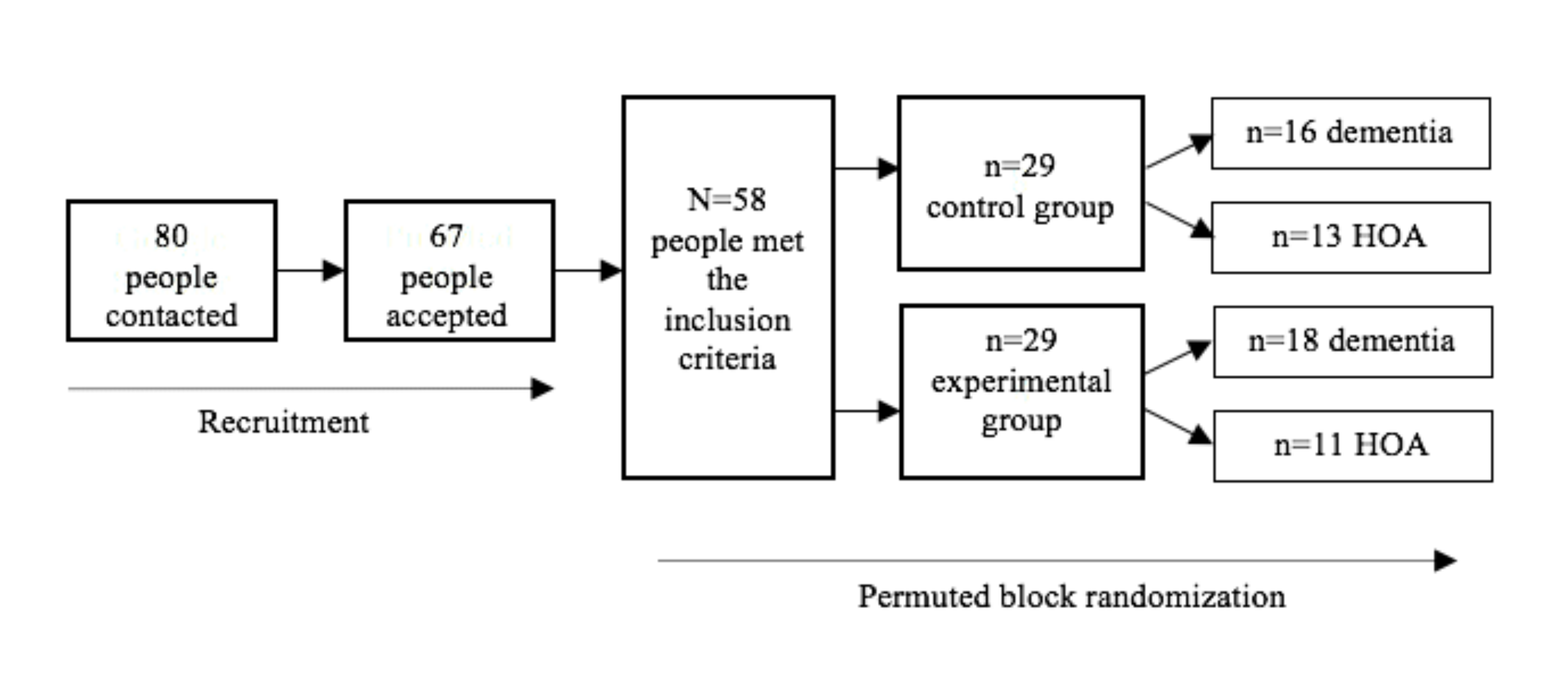
Figure 1 Flow diagram of the recruitment and randomization process.
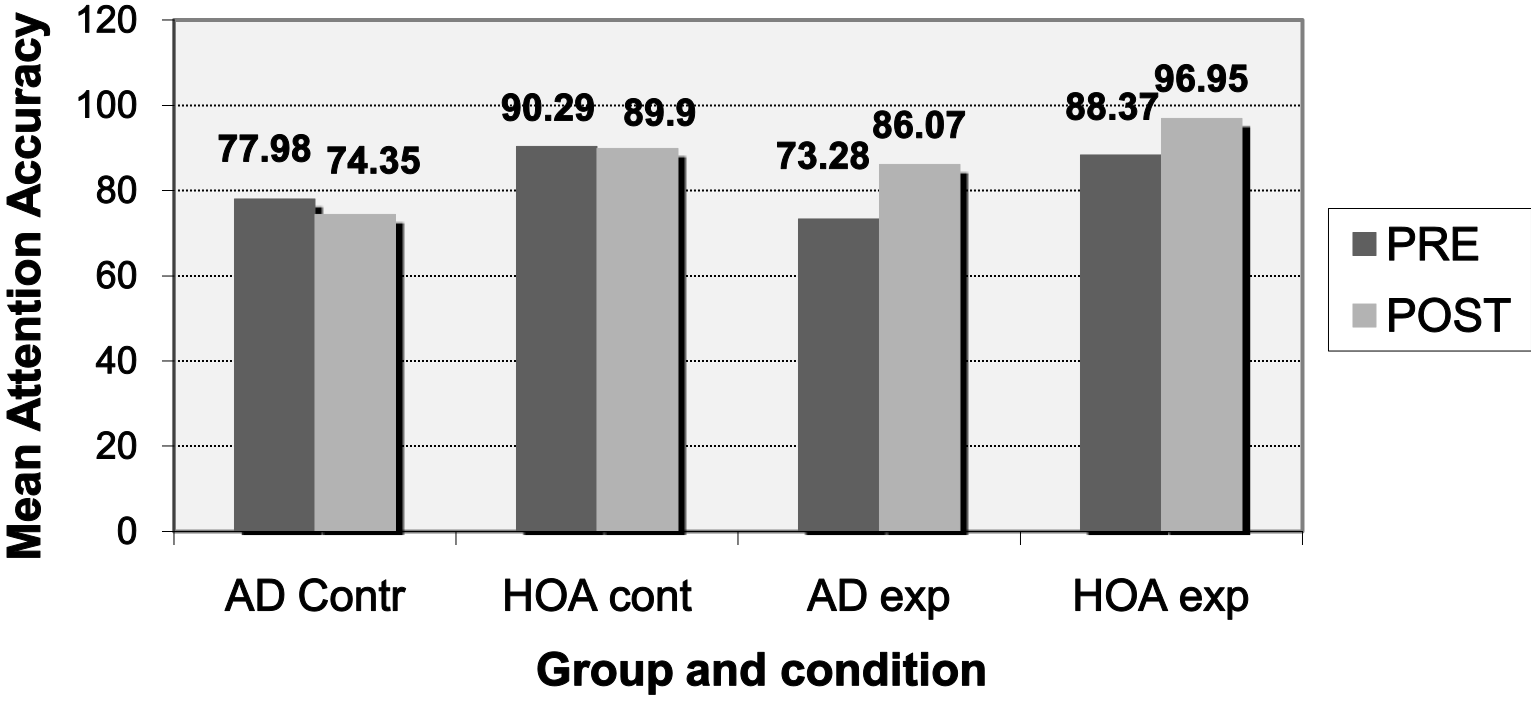
Figure 2 Mean visual search accuracy (Pr: % successes) for the experimental and control conditions in healthy older adults (HOA) and patients with Alzheimer´s disease (AD).
Materials
All participants provided personal information on their years of schooling, occupation, dietary habits, alcohol and drugs consumption, as well as on the presence of different disorders or diseases. Mini-Mental State Examination [30] and the SET-TEST verbal fluency [31] were used for the overall cognitive assessment of the participants and for ensuring that healthy older people did not present any cognitive impairment. In order to measure the efficiency of progressive music activation group, attention capacity was assessed through the adapted version of the visual search task in both the experimental and control groups before the beginning of group sessions and one week after the end of the intervention [1]. This visual search task was specifically adapted for evaluating attention capacity in progressive music activation intervention. The test itself consists of two parts: the first part, with 8 trials, lies in finding a green T letter from among other distracting letters; the second part, with 22 trials, lies in looking for a green N letter and for all letters in blue from among other distracting letters. The number of distracting letters varies in both parts of the test and may go from zero, four or fourteen to twenty-nine stimuli. The task was run on colour plates with 17.3 x 10.60 cm area, at an 80 cm distance from the eyes of the participants.
The selection procedure for music pieces for the present intervention was based on the indications found in this respect in literature, so that to strike a balance between quick and slow pieces. The music pieces used during 12 intervention sessions are given in Supplementary material (Annex 2). Moreover, the application of Jacobson progressive relaxation techniques pursues the aim to achieve a receptive state in the person before the beginning of the music intervention, through assuring relaxation by respiration, tension and relaxation of different body parts and visualization of pleasant scenes (Annex 3).
Study design and procedure
The participants who met inclusion criteria were randomly assigned to either intervention group or non-intervention group. An expert neuropsychologist assessed each subject with a brief neuropsychological battery in a 30-minute session prior to the experimental intervention (Table 1). No significant differences were found in base line between control group and intervention group for age (t (58) = -0.362 , p = 0.719), gender (t (58) = -.0463, p = 0.645), Isaacs (t (58) = -0.205, p = 0.839) and MMSE (t (58) = -0.263, p = 0.794).
Although the education level showed significant differences between control group and intervention group, we assume that this variable did not affect the results since the only two participants with high education (university level) belonged to the intervention group of healthy elderly, Education level (t (58) = -2,873, p = 0.006)
No significant differences were observed in base line between dementia group and healthy group for age (t (58) = -1.306, p = 0.197), gender (t (58) = -0.180, p = 0.858) and Education level (t (58) = 1.147, p = 0.256).
Once assessment was completed, we moved to the experimental phase. At that stage, participants held a preliminary assessment individual session, during which the visual search task was run. Following the preliminary session, those participants who had been assigned to intervention group assisted to 12 group intervention sessions, with a frequency of twice per week (Tuesday and Thursday) and 30-minute duration each. All participants were exposed to the same music and activation exercises. Intervention was carried out in the activity hall of the center, were group activities are normally performed. The two groups received the intervention separately (AD group and NPS group). The person in charge of sessions, a neuropsychologist specialized in music therapy (not the same neuropsychologist who assessed the participants before), was always the same. All sessions followed alike content structure: relaxation (5 min), auditory stimulation (20 min) and relaxation (5 min). The applied relaxation method was Jacobson’s progressive muscle relaxation technique. After the first relaxation, participants listened to music during the 20 minutes of auditory stimulation. Before starting, subjects were asked to seat themselves comfortably and to listening to music. In the absence of an objective measure of auditory acuity, all of them were asked to provide information on the point at the beginning of each session in order to adjust the volume to a comfortable and clearly audible level. The minimum selected volume for presenting audio tracks was between 60 and 65 decibels (dB), while the maximum selected volume for presenting audio stimuli was between 80 and 85 decibels (dB). The persons who did not receive intervention participated as usual in a conversation group activity. At the end of the intervention, one week after the 12th session, all participants were assessed through the visual search task in order to check the effect of the therapy (Annex 1).
|
Annex 1: Organization and intervention material. |
||||||
|
Parts
Sessions |
Relaxation |
Auditive stimulation |
Relaxation |
|||
|
Music |
Exercise |
Music |
Exercise |
Music |
Exercise |
|
|
1 |
“Agua y olas” |
R1,R2 |
G.F. Handel-Salomon - Sinfonia, Act 3, Corelli-Op.6 Concerto N° 10 (4_6) (Fabio Biondi), Corelli-Op.6 Concerto N° 12 (2_5) (Fabio Biondi) |
E1,E2 |
“Sonidos de la naturaleza” |
R1,R2 |
|
2 |
“Agua y olas” |
R1,R3 |
Álbum: “Breakthrough For Peak-Performance” |
E1,E2 |
“Brisas del mar” |
R1,R3 |
|
3 |
“Agua y olas” |
R1,R4 |
Álbum: “Illumination for Peak-Performance” |
E1,E2 |
“Azul profundo” |
R1,R4 |
|
4 |
“Agua y olas” |
R1,R5 |
Álbum: “Seasons At Roberts Mountain” |
E1,E2 |
“Zen garden” |
R1,R5 |
|
5 |
“Agua y olas” |
R1,R6 |
Álbum: Einstein's Dream” |
E1,E2 |
“Fondo del mar” |
R1,R6 |
|
6 |
“Agua y olas” |
R1,R7 |
Álbum: “Indigo For Quantum Focus” |
E1,E2 |
“El bosque” |
R1,R7 |
|
7 |
“Agua y olas” |
R1,R8 |
Álbum: “Baby Einstein - Baby Galileo” |
E1,E2 |
“Relaxing piano” |
R1,R8 |
|
8 |
“Agua y olas” |
R1,R9 |
Álbum: “Mozart Effect” |
E1,E2 |
“Cascadas relajación” |
R1,R9 |
|
9 |
“Agua y olas” |
R1,R10 |
Álbum: “Baroque Garden” |
E1,E2 |
“Canto de aves” |
R1,R10 |
|
10 |
“Agua y olas” |
R1,R11 |
Horowitz-Liszt Consolation No. 3, Chopin - Nocturno No. 2. |
E1,E2 |
“Brisa marina” |
R1,R11 |
|
11 |
“Agua y olas” |
R1,R2 |
Beethoven - Piano sonata #14 (moonlight). |
E1,E2 |
“Flauta japonesa” |
R1,R2 |
|
12 |
“Agua y olas” |
R1,R11 |
Chopin - Sonata en si bemol menor Op 35 (3er Mov - Marcha Funebre). |
E1,E2 |
“Fantasy Island” |
R1,R11 |
Statistical analyses
We analyzed the differences in the performance on the visual search task before and after the intervention in both healthy adult subjects and patients with Alzheimer’s disease (Table 2). A 2x2x2 between and within-factor ANOVA with the average of performance on the visual search task (% of correct answers) as dependent variable was applied. The analyzed factors are: assessment time (pre and post intervention), progressive music activation (intervention group and control group) and experimental group (NPS and AD).
RESULTS
The ANOVA analyses showed significant main effects due to the group (F (1, 54) = 27.85, p = 0.000), pointing at that healthy elderly (91.38%) had performed better on the attention task than the AD patients (77.92%, p = 0.000) under all conditions. Differences were also found due to the assessment time (F (1, 54) = 12.75, p = 0.001), pointing at a better performance on the attention task after the intervention (86.82%) than before the intervention (82.48%, p = 0.001). Interaction effects were found between the assessment time and progressive music activation intervention (F (1, 54) = 27.29, p = 0.000). Significant differences were observed between the pre-time of assessment (80.82%) and the post-time of assessment (91.51%) among those who received the intervention (F (1, 54) = 37.754, p = 0.000), independently of having AD or NPS or not. No differences were found between the two instances (84.13% versus 82.12%) for participants who did not follow the intervention (F (1, 54) = 1.401).
Post-hoc tests were carried out to further analyse this interaction separately for AD and NPS groups, since there are differences between the groups in their cognitive function. Both AD (p = 0.005) and NPS (p < 0.05) groups gave differences between pre-intervention span and post-intervention span; no differences were found for control groups who had not undergone the intervention. These results confirm the efficicacy of the intervention in both patients with dementia and elderly without dementia (Figure 2).
No differences were found between participants who had followed the intervention (80.82%) and those who had not (84.13%) at the time prior to the intervention (F (1, 54) = 1.290), but we did find differences (91.51% versus 82.12%) at the second assessment (F (1, 54) = 11.788, p = 0,01), regardless of whether these persons had AD or NPS.
Those participants who received the intervention showed a significantly better performance after participation than those participants who had not followed the intervention. Interaction effects were found between the assessment time and the group of elderly (F (1, 54) = 27.297, p = 0.000). However, no differences were found due to the main effect of the intervention (F(1,54) = 1.418, p = 0.239), pointing at that participants who received the intervention, compared with those who did not, perform equally if we do not consider other factors, such as assessment time or group of elderly.
Those participants who received the intervention showed a significantly better performance after participation than those participants who had not followed the intervention. Interaction effects were found between the assessment time and the group of elderly (F (1, 54) = 27.297, p = 0.000). However, no differences were found due to the main effect of the intervention (F(1,54) = 1.418, p = 0.239), pointing at that participants who received the intervention, compared with those who did not, perform equally if we do not consider other factors, such as assessment time or group of elderly.
No interaction effect was found between the variables of group of elderly and progressive music activation (F (1, 54) = 0.041) or assessment time (F (1, 54) = 2.347).
DISCUSSION
The data obtained in this study are congruent with other studies of similar characteristics [32-35]. In this sense, regular musical leisure activities can have long-term cognitive, emotional, and social benefits in mild/moderate dementia and could therefore be used in dementia care and rehabilitation. In the same way, a music-based exercise programme in a group of patients with moderate to severe dementia [8] suggests a beneficial effect on cognition and in quality of life [36]. Further studies are needed to confirm these findings.
The characteristics of the music stimuli used in this study deserve special consideration. As it has been previously mentioned, the type of the chosen classical melodies could have improved subjects concentration during the stimuli presentation [17,18] what implies a fuller attention. As for the healthy older adults, who maintain “intact” cortical circuits, the results of our study show that progressive music activation is a promising tool for relieving the attention impairment associated with ageing. Thereby, it is essential to keep on working on in the search of new non pharmacological interventions dealing with the strengthening of cognitive processes associated with selective attention in patients with AD.
However, the lack of methodologically valid studies which support scientifically the efficacy of musical therapies on cognitive variables has been harshly criticized [37]. Particularly, it has been stressed on the placebo effects problems and the problems of general stimulation, what occurs with the majority of therapies, specifically among the elderly residents in institutions.
The major limitation of this study is the small sample size. In addition, another constraint of this study consists in including persons from different retirement homes of the same town.
One more remaining issue to explore is the maintenance of the training effects. How long are the effects of the intervention sustained once the stimulation is finished? Additional follow-up studies are required to answer this question.
In our future studies, we will continue to recruit subjects from a more extensive geographical area and from different settings (hospitals, day care centers, etc.), in order to ensure the representativeness, extrapolation and validity of the results. In addition, it will be needed to apply long-term assessment to confirm the effects of the intervention in time.
|
Table 1: Demographic and standard neuropsychological test data by group. |
|||||
|
|
AD control |
AD exp. |
HOA control |
HOA exp. |
Total |
|
Sample size (N) |
16 |
18 |
13 |
11 |
58 |
|
Gender (M:F) |
3M/13F |
2M/16M |
1M/12F |
2M/9F |
8M/50F |
|
Age (years) |
82 (7.193) |
80.74 (10.021) |
76.23 (10.756) |
79.75 (12.248) |
79.90 (9.984) |
|
Education level |
5.25 (2.049) |
6.57 (2.523) |
5.53 (1.664) |
8.00 (2.954) |
6.28 (2.498) |
|
MMSE |
17.25 (5.495) |
17.63 (3.715) |
25.92 (2.216) |
27.75 (2.454) |
21.35 (5.997) |
|
SET-TEST |
24.62 (9.783) |
24.89 (9.091) |
35.00 (4.490) |
37.50 (1.977) |
29.533 (9.345) |
|
*Standard deviation is given in italics. Education level: 0 = no education; 1 = primary schooling; 2 = secondary schooling. Abbreviations: AD: Alzheimer´s Disease; exp: Experimental Group; HOA: Healthy Older Adults; MMSE: Mini-Mental State Examination |
|||||
|
Table 2: Hits percentage in selective attentional task. |
||
|
|
PRE |
POST |
|
AD control |
77.98 (10.35) |
74.35 (13.77) |
|
AD exp. |
73.28 (14.40) |
86.07 (11.93) |
|
HOA control |
90.29 (4.87) |
89.90 (4.46) |
|
HOA exp. |
88.37 (9.97) |
96.95 (3.65) |
|
*Standard deviation is given in italics. The results show the percentage of the average of corrects answers (% of correct answers) for the attention test before (PRE) and after (POST) the intervention. Abbreviations: PRE: Before the Intervention; POST: Moment after the Intervention; AD: Alzheimer´s Disease; exp: Experimental Group; HOA: Healthy Older Adults |
||
CONCLUSION
To our knowledge, this is the first study of the effects of progressive music stimulation on the selective attention in elderly and people with dementia.
The main objective of this research was to determine the degree to which progressive music activation could be used for improving attentional capacity of visual search in patients with AD and in healthy elderly. The obtained results confirm our hypothesis on that both AD patients and healthy older adults receiving progressive music activation intervention show a better performance on the attention task than the control group; therefore, the intervention achieved its objectives. Consequently, these data prove the effectiveness of the intervention and suggest that progressive music stimulation enhances selective attention.
Despite the aforementioned limitations, we strongly believe that given results and their implications might be useful for further studies on selective attention improvement in elderly and persons with dementia. In this way, it is possible to work on enhancing attentional quality in elder people and people with dementia. Our study found that progressive music activation intervention can improve attention deficits in people with dementia; therefore, we recommend implementing such intervention with standardized methods for measuring different physiological indexes in future studies. Understanding the nature of music processing and attention in AD patients can allow for developing effective and integral therapies for tackling the disease, which is becoming more prevailing. It will be additionally interesting to test the importance of relaxation on the music effect, since it is the relaxation itself, which allows for paying attention to auditory stimulus. For this reason, we recommend gerontological centers and centers of attention to persons with dementia to adopt the procedure of groups of progressive music activation intervention as a routine activity.
ACKNOWLEDGEMENTS
We are very thankful to the residents who shared with us their experience and showed us the important role of music and progressive activation in their lives. We would also like to express our gratitude to the centres’ assistance personnel, as well as to all students who backed this study. Our special appreciation is for the State Reference Centre of Attention for persons with Alzheimer’s and other Dementias, as well as to the nursing homes Jesán and Sauvia from Salamanca, for their unconditional support.
Session 1. G.F. Handel-Salomon - Sinfonia, Act 3, 03:15mn.; Corelli-Op.6 Concerto N° 10 (4_6) (Fabio Biondi) 12:26mn; Corelli-Op.6 Concerto N° 12 (2_5) (Fabio Biondi), 10:22mn;
Session 2. Wolfgang Amadeus Mozart - Piano Concerto No. 21 - Andante, 05:51mn, Mozart-The Marriage of Figaro, 04:50 mn, Mozart Symphony #40 in G Minor, K 550 - 1. Molto Allegro, 08:15 mn; Turkish March Mozart, 04:02 mn.
Session 3. Four Seasons ~ Vivaldi: Spring, 10:00 mn, Summer, 10:27mn & Autumn, 11:13mn.
Session 4. Álbum: “Einstein’s Dream”, 29:09mn.
Session 5. Chopin - Nocturne In E Flat Major, Op.9 No.2, 04:08mn, Schubert: Drei Klavierstücke -- D946, 23:25mn.
Session 6. Álbum: “Baroque Garden”. Songs 1 to 6, 23:50mn. Hemi-Sync®.
Session 7. Tchaikovsky : Symphony No.3 in D major, Op.29 “Polish”, 20:00 first minutes.
Session 8. Verdi - Nabucco - Overture, 07:53mn, Verdi - Marcha Triunfal de Aida, 06:03mn, Dmitri Shostakovich - Waltz No. 2, 03:50mn, Johann Sebastian Bach - Orchestral Suite No. 3 D-dur (BWV 1068), 05:51mn.
Session 9. Álbum: “Mozart Effect”. Songs 1 to 5, 24:00mn. Hemi-Sync®.
Session 10. Horowitz-Liszt Consolation No. 3, S 172, 04:26mn, Chopin - Nocturno No. 2.05:00mn. Mozart: 12 Variations on “Ah, vous dirai-je Maman” KV 265 for Piano, 12:44mn, Alonso Lobo - Versa est in luctum, 04:48mn.
Session 11. Beethoven - Piano sonata No.14 (moonlight).15:00mn, Beethoven-For Elise, 02:57mn, Schubert - Ave Maria, 06:16mn.
Session 12. Chopin - Sonata en si bemol menor Op 35 (3er Mov - Marcha Funebre), 08:59mn, Chopin - Nocturne in C sharp Minor (No.20), 04:04mn, Chopin - Spring Waltz, 04:22mn, Maurice Ravel - Pavana para una infanta difunta, 05:54mn.
Relaxation session. Música utilizada para comenzar y finalizar la sesión: “Agua y olas” ,05:00mn y “Relaxing piano music”, 05:00mn
Exercise varities used during group session for guided progressive activation
- R1. The arms are placed on the legs in restful position; attention is focused on breathing. For inspiring, the air is taken energetically so that to feel the lungs in. Participants imagine that they aspire fresh and pure air, which intensivelly enters in their interior and leaves a good feeling. For expiring, participants breathe out and listen to the air passing by the mouths. Participants start to feel a slight relaxation in their bodies. This respiration exercise should be repeated three times.
- R2. The arms are slowly lifted and separated with manifest slowness from the legs. These movements are almost imperceptible; the participants must progressively notice the weight of the arms. The arms will stay lifted for five seconds; then, participants will carry the opposite movement, with the arms moved towards the legs in a slow way. Participants will have a rest for some seconds, during which they will try to think about the difference in arm sensations before and after the exercise. Arms movements are to be repeated three more times. After the exercise, a short pause is to be commited. For one minute approximately, the participants are to comment in turns their feeling while carrying out this exercise.
- R3. It is a joint respiration and arm movement exercise. For inspiring, the participants lift the arms and focus on both breathing and movement. The arms are maintained lifted for some seconds and go back slowly to the initial position of arms on the legs; at the same time, the air is expelled from lungs with force. Participants may feel heaviness, heat or tingling in their arms, what is normal after this exercise. Participants are suggested to think in feeling refreshed, since mental reinforcement can help in achieving physical relaxation.
- R4. The procedure is the same as in R2; now, however, the exercise will begin with the right arm and, then, with the left. Three repetitions for both arms are to be performed. Attention will be paid to the difference in tension perception before and after the exercise.
- •R5. The fists are closed as mush as possible during several seconds. Participants are to be aware of the tension that this exercise produces. Hereunder, participants open the fists and relax them completely. Differences in feeling are percieved. The exercise is to be repeated three times.
- •R6. Participants take the position of “making weights”: their arms are twisted upwards at elbows. The muscles are tighthened in the front part of the arms. Participants maintain this position. Thereon, the arms are expanded and dropped, and felt relaxed while suspended lengthwise the body. This exercise is repeated three times. Initial tension is compared with the feeling after the exercise.
- R7. The shoulders are shrugged and lifted towards the nape as much as possible, so that to fell tension. This position is maintained during five seconds; after that, participants relax, drop and spread their shoulders. Relaxation is felt during several seconds. This exercise is repeated three times.
- R8. Participant’s intake air by nose and, at the same time, raise their eyes towards the ceiling. In this way, they tighten their necks while air is entering into the lungs. For expiration, participants breathe through the mouth and, at the same time, look towards the floor. In this way, they relax and release their necks. The exercise is repeated three times.
- R9. Eyes are closed tightly. All muscles surrounding them are tightened and eyebrows are frown. This position is maintained for five seconds; thereon, participants feel their eyebrows dropped and open their eyes slowly, so that to feel relaxed. The exercise is repeated three times.
- R10. Participants intake air by nose and, at the same time, turn slowly their neck to the right. They maintain this position during five second and turn slowly the neck back, releasing the tension from their muscles. The following three repetitions alternate shifts to the right and to the left.
- R11. Participants close their eyes and forget all their worries. They imagine a place they would like to be at the moment: a restful and calm place. Participants are encouraged to display that place vividly, so that to hear, smell or feel it. Sensory details are added while music is playing in the background. Participants may smell the sea and the breeze, they may hear the waves crashing on the sand. When the exercise is finished, participants open the eyes and talk about their feelings during the visualisation.
It is at this point that the body and the mind are ready to receive auditory stimulation, which will increase the level of alert and consciousness. The stimulation will be carried out through listening to Barocco music, in particular, to such composers as Vivaldi, Corelli, Mozart, Händel, etc., for approximately twenty minutes. At the beginning, there will be a period for active listening (E1); thereon, participants will be offered to volunterily share and express their feelings under music effect, and their memories and emotions in this period (E2).
Before the end, the progressive activation technique will be applied again for five minutes. Execises may be slighlty changed to favour progressive adaptation to the outside.
REFERENCES
- Leonards U, Sunaert S, Van Hecke P, Orban GA. Attention mechanisms in visual search -- an fMRI study. J Cogn Neurosci. 2000; 12: 61-75.
- Zatorre RJ, Chen JL, Penhune VB. When the brain plays music: auditory-motor interactions in music perception and production. Nat Rev Neurosci. 2007; 8: 547-558.
- Särkämö T, Tervaniemi M, Huotilainen M. Music perception and cognition: development, neural basis, and rehabilitative use of music. Wiley Interdisciplinary Reviews: Cognitive Science. 2013; 4: 441-451.
- Gerdner LA. Individualized music for dementia: Evolution and application of evidence-based protocol. World J Psychiatry. 2012; 2: 26-32.
- Guetin S, Charras K, Berard A, Arbus C, Berthelon P, Blanc F, et al. An overview of the use of music therapy in the context of Alzheimer's disease: a report of a French expert group. Dementia (London). 2013; 12: 619-634.
- Ridder HM, Stige B, Qvale LG, Gold C. Individual music therapy for agitation in dementia: an exploratory randomized controlled trial. Aging Ment Health. 2013; 17: 667-678.
- Sakamoto M, Ando H, Tsutou, A. Comparing the effects of different individualized music interventions for elderly individuals with severe dementia. Int Psychogeriatr. 2013; 25: 775-784.
- Van de Winckel A, Feys H, De Weerdt W, Dom R. Cognitive and behavioural effects of music-based exercises in patients with dementia. Clinical Rehabilitation. 2004; 18: 253-260.
- Thaut MH. Rhythm, music, and the brain: Scientific foundations and clinical applications. 2005; 7.
- Särkämö T, Tervaniemi M, Laitinen S, Forsblom A, Soinila S, Mikkonen M, et al. Music listening enhances cognitive recovery and mood after middle cerebral artery stroke. Brain. 2008; 131: 866-876.
- McGuinness B, Barrett SL, Craig D, Lawson J, Passmore AP. Attention deficits in Alzheimer's disease and vascular dementia. J Neurol Neurosurg Psychiatry. 2010; 81: 157-159.
- Romberg C, Bussey TJ, Saksida LM. Paying more attention to attention: towards more comprehensive cognitive translation using mouse models of Alzheimer's disease. Brain Res Bull. 2013; 92: 49-55.
- Perry RJ, Watson P, Hodges JR. The nature and staging of attention dysfunction in early (minimal and mild) Alzheimer’s disease: relationship to episodic and semantic memory impairment. Neuropsychologia. 2000; 38: 252-271.
- Lustig C, Hasher L, Zacks RT. Inhibition deficit theory: recent developments in a new view. In Gorfein DS, MacLeod CM. The place of inhibition in cognition. American Psychological Association. 2007; 145-162.
- McDowd JM, Shaw RJ. Attention and aging: A functional perspective. In F. I. M. Craik yT. A. The handbook of aging and cognition. 2000; 221-292.
- Benke T, Karner E, Petermichl S, Prantner V, Kemmler G. Neuropsychological deficits associated with route learning in Alzheimer disease, MCI, and normal aging. Alzheimer Dis Assoc Disord. 2014; 28: 162-167.
- Bernardi L, Porta C, Casucci G, Balsamo R, Bernardi NF, Fogari R, et al. Dynamic Interactions Between Musical, Cardiovascular, and Cerebral Rhythms in Humans. Circulation. 2009; 119: 3171-3180.
- Trappe HJ. The effects of music on the cardiovascular system and cardiovascular health. Heart. 2010; 96: 1868-1871.
- Khalfa S, Isabelle P, Jean-Pierre B, Manon R. Event-related skin conductance responses to musical emotions in humans. Neurosci Lett. 2002; 328: 145-149.
- Bernardi L, Porta C, Sleight P. Cardiovascular, cerebrovascular, and respiratory changes induced by different types of music in musicians and non-musicians: the importance of silence. Heart. 2006; 92: 445-452.
- Gomez P, Danuser B. Relationships between musical structure and psychophysiological measures of emotion. Emotion. 2007; 7: 377-387.
- Khalfa S, Bella SD, Roy M, Peretz I, Lupien SJ. Effects of relaxing music on salivary cortisol level after psychological stress. Ann N Y Acad Sci. 2003; 999: 374-376.
- Leardi S, Pietroletti R, Angeloni G, Necozione S, Ranalletta G, Del Gusto B. Randomized clinical trial examining the effect of music therapy in stress response to day surgery. British journal of surgery. 2007; 94: 943-947.
- Sokhadze EM. Effects of music on the recovery of autonomic and electrocortical activity after stress induced by aversive visual stimuli. Appl Psychophysiol Biofeedback. 2007; 32: 31-50.
- Schubert E. Emotion felt by the listener and expressed by the music: literature review and theoretical perspectives. Front Psychol. 2013; 4: 837.
- Husain G, Thompson WF, Schellenberg EG. Effects of musical tempo and mode on arousal, mood, and spatial abilities. Music Perception. 2002; 20: 151-171.
- Schmidt LA, Trainor LJ. Frontal brain electrical activity (EEG) distinguishes valence and intensity of musical emotions. Cognition Emotion. 2001; 15: 487-500.
- Sloboda JA, Juslin PN. Psychological perspectives on music and emotion. Theory and research. 2001; 71-104.
- Thompson WF, Schellenberg EG, Husain G. Arousal, mood, and the Mozart effect. Psychol Sci. 2001; 12: 248-251.
- Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975; 12: 189-198.
- Isaacs B, Akhtar AJ. The set test: a rapid test of mental function in old people. Age Ageing. 1972; 1: 222-226.
- Khakha DC, Satapathy S, Dey AB. Impact of Jacobson Progressive Muscle Relaxation (JPMR) and Deep Breathing Exercises on Anxiety, Psychological Distress and Quality of Sleep of Hospitalized Older Adults. J Psychosocial Res. 2015; 10: 211-223.
- Särkämö T, Tervaniemi M, Laitinen S, Numminen A, Kurki M, Johnson JK, et al. Cognitive, Emotional, and Social Benefits of Regular Musical Activities in Early Dementia: Randomized Controlled Study. Gerontologist. 2014; 54: 634-650.
- Scheufele PM. Effects of progressive relaxation and classical music on measurements of attention, relaxation, and stress responses. J Behav Med. 2000; 23: 207-228.
- Simmons-Stern NR, Budson AE, Ally BA. Music as a memory enhancer in patients with Alzheimer's disease. Neuropsychologia. 2010; 48: 3164-3167.
- Van Bruggen-Rufi M, Vink A, Achterberg W, Roos R. Improving quality of life in patients with Huntington s disease through music therapy: A qualitative explorative study using focus group discussions. Nordic J Music Ther. 2017; 1-23.
- Vink AC, Bruinsma MS, Scholten RJ. Music therapy for people with dementia. The Cochrane Library. 2004.









































































































































