Morphometric Measurements of Supraorbital and Infraorbital Foramen in Dry Skulls of Local Population
- 1. Department of Anatomy, King Edward Medical University, Pakistan
- 2. Department of Anatomy, Rawalpindi medical college, Pakistan
Abstract
Background: Superior orbital region is used for supraorbital nerve blocks for multiple procedures such as closure of wounds, biopsies, scar revisions, and other facial cosmetic procedures hence a thorough knowledge of this region is essential for the clinicians to effectively anaesthetize the supraorbital nerve. Infraorbital nerve is a branch of the maxillary nerve which is second stem of the trigeminal nerve. Supraorbital foramen/notch and infraorbital foramen are important anatomic landmarks from which important nerves exit from the skull.
Results: All the skulls showed supraorbital foramen/notch and infraorbital foramen on both sides. There is no difference of measurements of right and left orbits. But racial differences exist among African, Asian and Caucasian population.
Conclusion: Precise morphometric details of supraorbital foramen/notch and infraorbital foramen would be beneficial for various diagnostic, therapeutic endoscopic, anesthetic and surgical procedures.
Keywords
Supraorbital foramen; Infraorbital foramen; Skull
Citation
Rasheed A, Hina M, Tafweez R (2019) Morphometric Measurements of Supraorbital and Infraorbital Foramen in Dry Skulls of Local Population. JSM Anat Physiol 4(1): 1021.
ABBREVIATIONS
KEMU : King Edward Medical University; RSOFTD: Right Supraorbital Foramen Transverse Diameter; RSOFVD: Right Supraorbital Foramen Vertical Diameter; RSOFMLD: Right Supraorbital Foramen Midline Distance; LSOFTD: Left Supraorbital Foramen Transverse Diameter; LSOFVD: Left Supraorbital Foramen Vertical Diameter; LSOFMLD: Left Supraorbital Foramen Midline Distance; RIOFTD: Right Infraorbital Foramen Transverse Diameter; RIOFVD: Right Infraorbital Foramen Vertical Diameter; RIOFMLD: Right Infraorbital Foramen Midline Distance; LIOFTD: Left Infraorbital Foramen Transverse Diameter; LIOFVD: Left Infraorbital Foramen Vertical Diameter; LIOFMLD: Left Infraorbital Foramen Midline Distance
INTRODUCTION
The supraorbital margin on both sides formed by frontal bone is notched or canalized near its medial end to form the supraorbital notch/foramen through which the supraorbital nerve and vessel exit the skull [1]. The supraorbital nerve is a branch of the first division of the ophthalmic branch of the trigeminal nerve [2]. Superior orbital region is used for supraorbital nerve blocks for multiple procedures such as closure of wounds, biopsies, scar revisions, and other facial cosmetic procedures hence a thorough knowledge of this region is essential for the clinicians to effectively anaesthetize the supraorbital nerve [3]. A accurate knowledge of presence of either supraorbital notch or foramen and their exact location is essential for prevention of supraorbital neuralgia, and entrapment nerve syndromes which can result from injury due to excessive dissection resulting in scarring, close to the neurovascular bundle [4].
Infraorbital nerve is a branch of the maxillary nerve which is second stem of the trigeminal nerve. After it exits from skull through foramen rotundum, maxillary nerve enters into the pterygopalatine fossa and from there it goes to the posterior teeth by giving its palatine and nasal branches [5]. When, it enters into the orbit from inferior orbital fissure then referred as infraorbital nerve. Infraorbital nerve passes through infraorbital groove and infraorbital canal and extended to the skull via the infraorbital foramen [6]. Infraorbital nerve injuries might occur in the anterior and superior nasal walls during the surgical treatments such as rhinoplasty, tumor surgery and many types of fracture union surgeries [7].
Supraorbital foramen/notch and infraorbital foramen are important anatomic landmarks from which important nerves exit from the skull. These nerves are involved in pain syndromes and various nerve blocks during tissue infiltration in maxillofacial and cosmetic surgeries. Various studies showed differences in dimensions and location of these foramen in different racial groups [8]. Little information is available concerning the morphometric details of this foramen in our local Pakistani population. This study will be helpful in knowing exact measurements of this facial foramen in relation to surgicallyencountered anatomic landmarks. Precise morphometric details of supraorbital foramen/notch and infraorbital foramen will be beneficial for various diagnostic, therapeutic endoscopic, anesthetic and surgical procedures.
MATERIALS AND METHODS
This study was carried out in Anatomy department of K.E.M.U. Lahore. 32 dry human adult skulls were taken. Number of Supraorbital foramen/Notch and Infraorbital Foramen, maximum transverse and vertical diameters and their distances from the midline were measured by digital vernier calipers in millimeters. In case of supraorbital foramen/Notch distance from the nasal midline was measured. In case of infraorbital foramen distance from the maxillary midline was measured. Mean and standard deviation were calculated from the data by using SPSS version 18.0.
RESULTS AND DISCUSSION
All the skulls showed supraorbital foramen/notch and infraorbital foramen on both sides for supraorbital foramen/ notch as shown in table. All the skulls showed single infraorbital foramen on both sides.
Right sided supraorbital foramen of all skulls showed mean transverse diameter 2.420+.451mm while left sided supraorbital foramen showed 2.139+.391mm. Right sided supraorbital foramen of all skulls showed mean vertical diameter 3.649+.687 mm while left sided foramen showed 3.489+.651mm. Right sided infraorbital foramen showed mean transverse diameter 2.858+.633mm and left sided foramen showed mean transverse diameter 3.112+.823 mm. Right sided infraorbital foramen showed mean vertical diameter 4.199+.732 mm and left sided foramen showed 4.229+.887mm (Figure 1 and 2).
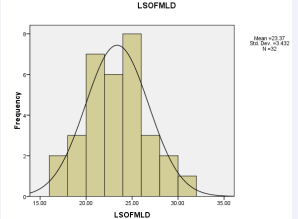
Figure 1: Right sided supraorbital foramen of all skulls showed mean transverse diameter.
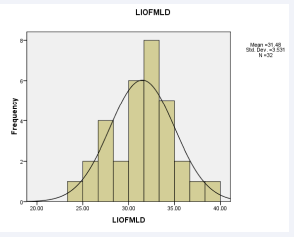
Figure 2: left sided supraorbital foramen of all skulls showed mean transverse diameter.
The accurate position of the supraorbital and infra orbital foramina is very important for the anesthetists and surgeons while giving nerve block. It is an important landmark for both diagnostic and surgical procedures. Any injury to the nerve bundle emerging from the foramen may result in complications. Therefore, head and neck, maxillo-facial surgeons and anesthetists should have a good knowledge regarding the morphological parameters and the variations of supraorbital and infra orbital foramina.
In our study there was no significant difference in dimensions of foramen from right and left sides of skull, same results also showed by Sithiporn et al., in their study [9]. Occurrence of supraorbital notch is more frequent in our study (75%) and in previous studies showed 55.56% and 50.5% [10,11]. Ashwini et al., showed more frequency of supraorbital notches in their study [12]. Occurrence of multiple supraorbital foramina was 7.8% in contrast with previous studies [10,11,13] (Figure 3and 4) (Tables 1-3).
Table 1: Frequency of supraorbital foramen as single, multiple foramen and supraorbital notch.
| Frequency | Percentage | |
| Single foramen | 11 | 17.1875 |
| Notch | 48 | 75 |
| Multiple foramen | 5 | 7.8125 |
| Total | 64 | 100 |
Table 2: Supraorbital foramen measurements.
| RSOFTD | RSOFVD | LSOFTD | LSOFVD | RSOFMLD | LSOFMLD | ||
| N | Valid | 32 | 32 | 32 | 32 | 32 | 32 |
| Missing | 0 | 0 | 0 | 0 | 0 | 0 | |
| Mean | 2.4206 | 3.6491 | 2.1397 | 3.4897 | 24.5644 | 23.3738 | |
| Std. Deviation | .45146 | .68767 | .39087 | .65134 | 3.30545 | 3.43240 |
Table 3: Infraorbital foramen measurements.
| RIOFTD | RIOFVD | LIOFTD | LIOFVD | RIOFMLD | LIOFMLD | ||
| N | Valid | 32 | 32 | 32 | 32 | 32 | 32 |
| Missing | 0 | 0 | 0 | 0 | 0 | 0 | |
| Mean | 2.8581 | 4.1991 | 3.1128 | 4.2291 | 32.2219 | 31.4831 | |
| Std. deviation | .63273 | .73291 | .82363 | .88782 | 3.73067 | 3.53110 |
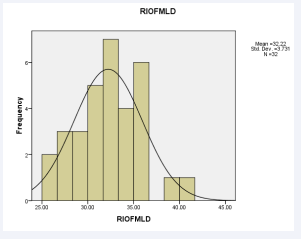
Figure 3: Right sided infraorbital foramen showed mean transverse diameter
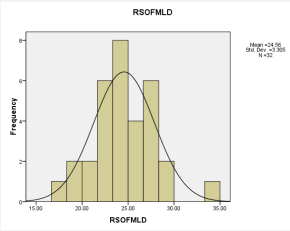
Figure 4: Left sided infraorbital foramen showed mean transverse diameter.
Single infraorbital foramen was observed on both sides in our study different from other studies which showed 3.6% in Thai population. Mean diameters of supraorbital foramen/notch and infraorbital foramen were not significantly different among Asians [10], but these vary among White and Black populations [9,14]. Our study revealed midline distances for supraorbital and infraorbital foramen were in consistent with results observedin Thai and Korean population [10,15]. The knowledge of dimensions of these anatomical landmarks in the present study may assist surgeons to localize these important facial openings, avoid injury to the neurovascular bundles and facilitate surgical, local anesthetic and other invasive procedures.
CONCLUSION
It can be stated that the exact location of supraorbital foramen/notch is not constant and it varies between different racial groups and people of various regions. Supraorbital notch is observed more frequently as compared to the supraorbital foramen. Infraorbital foramen measurements vary among different races. Because of these variations of the exit points of the supraorbital and infraorbital nerves and its branches; all the surgical procedures involving the supraorbital and infraorbital rim and adjoining areas have to be performed very carefully with the awareness of probable variations.
ACKNOWLEDGEMENTS
I am thankful to Allah Almighty who supported me in every aspect.
REFERENCES








































































































































