Clinical Response to Oral Ibandronate in Paget
- 1. Division of Endocrinology and Diabetes, Hospital Agamenon Magalhães- SUS / University of Pernambuco, Recife, Brazil
Abstract
Introduction: The main goals of treatment of Paget’s disease of the bone (PDB) are to restore normal bone metabolism, relieve bone pain and prevent future complications. Bisphosphonates have been used for several decades, as the class of choice for the treatment of PDB. Oral alendronate and risedronate are used in higher doses than those used for osteoporosis that is 30mg/day and 20 to 40mg/day for 2 and 6 months respectively. Pamidronate (60-180mg), ibandronate (2mg) and zolendronate (5mg) can also be used intravenously. There is no data on the treatment of PDB with oral ibandronate.
Objective: To evaluate the clinical and laboratory response of the treatment with oral ibandronate (150mg/month) for 6 months in 12 patients with PDB.
Methods: We evaluated the intensity of bone pain, the alkaline phosphatase (AP) and serum ß-cross-links-C telopeptide (sCTX) in 12 patients with PDB, mean age 68.6 ± 11,2 years-old, serum AP 1.49 ± 0,98 times the upper limit of normal (ULN). sCTX was elevated in 10 patients (mean 2,13 ± 1,2 times ULN), before treatment.
Results: After 6 months of treatment, the mean reduction in sCTX was 65,24 ± 28,9%, reaching 80% in 7 patients. The mean reduction of sAP was 49,21 ± 37,9%, with all patients having normal values in sAP after treatment. There was a significant clinical response in all patients, with marked improvement in bone pain.
Conclusion: Our data demonstrate high efficacy of oral ibandronate in the treatment of PDB at equivalent doses used in the treatment of osteoporosis.
Keywords
• Paget’s disease of bone
• Ibandronate
• Alkaline phosphatase
• Pain relief
Citation
Voss L, Coimbra B, Bandeira F (2016) Clinical Response to Oral Ibandronate in Paget’s Disease of Bone. JSM Arthritis 1(3): 1018.
INTRODUCTION
Paget’s disease of bone (PDB) was first described in 1876 [1] by the English surgeon Sir James Paget [2,3] as a skeletal disorder characterized by excessive osteoclastic bone resorption [4,5], followed by an increase in osteoblastic activity [6,7], leading to the substitution of normal bone for disorganized bone [7], being weak in structure and prone to fractures and deformities [7]. The etiology is uncertain [8,9], with a possible combination of genetic [3,10] and environmental [3-5] factors. Some epidemiological studies showed a positive family history in up to 40% of affected patients [3,5]. The incidence increases with age and has slightly higher prevalence in males [11,12]. Rates vary from 0.7% to 4.6%. In the United States approximately 2–3% among individuals over age 55 years [12]. Marked geographical variation and a higher prevalence were noted in Western Europe, New Zealand, Australia and the United States being rarer in Asia, Africa and Eastern Europe [8-11]. In Brazil, predominantly affects patients of European descent [10-13]. In Recife, Brasil, one study showed a prevalence of 6.8/1,000 individuals and incidence rates of 50.3/10,000 patient-years. These figures are similar what have been reported from southern Europe [10-13].
Most patients are asymptomatic [2,11,12,14] and diagnosis is usually made by radiological abnormalities or elevated alkaline phosphatase [12,14]. The main clinical manifestation is bone pain [14], which occurs most often when related to complications. The most frequent complications include pathological fractures, bone deformities, secondary degenerative osteoarthritis, compression of nerves and hearing loss [8]. Sarcomatous degeneration although rare, at 0.4[8] to 1% [11], usually presents bad prognosis [8].
The goals of treatment are to relieve pain, prevent complications, decreased bone vascularization, achieving reduction in disease progression and bone remodeling, restoring the normal bone metabolism and inducing sustained biochemical remission [11,12].
The treatment of PDB has evolved considerably over the past decades with the use of medicine which promotes remission and prevents complications [11,12]. Bisphosphonates have a biological property to inhibit osteoclastic bone resorption [15- 18]. These drugs are currently the first choice of treatment for metabolic bone diseases such as osteoporosis, hypercalcemia of malignancy, bone metastases and PDB [17].
Oral alendronate is administered in larger doses than used to treat osteoporosis, in doses of 20 mg to 40 mg/day for 6 months [6,15]. It is more effective than pamidronate in patients previously treated with a bisphosphonate, however, alendronate and pamidronate are comparably effective in previously untreated patients [4,6,11,12]. Pamidronate induces a reduction of bone remodeling by 60- 70% [11]. It is used intravenously at a dose of 60 mg to 180mg [11,20,21]. As time passed, higher doses and shorter time of infusion were used and osteomalacia [11,21] nephropathies such as focal glomerulosclerosis, and cases of drug resistance were observed [7,11]. Risedronate is used in higher doses than those used for osteoporosis, 20 to 40mg/day for 2 and 6 months [11,22,23]. At doses of 30 mg/day for 2 months leads to normalization of sAP in 73% [7]. Zoledronic acid is a third generation potent bisphosphonate. It is used at a dose of 5mg, intravenously [5]. Osteonecrosis of the jaw has been reported with the use of zoledronic acid [24,25], however it has been associated with high doses and dental manipulation during treatment [11]. Ibandronate is a potent amino-bisphosphonate available in both oral [26] and intravenous (IV) [27,28] presentation. Preclinical studies have shown that ibandronate sodium is 2, 10, 50, 500 and 10,000 times respectively more potent than risedronate, alendronate and pamidronate, clodronate and etidronate in vitro [28]. Due to its high potency, a smaller amount of ibandronate would be required to effectively inhibit bone resorption than other oral bisphosphonates, in PDB. Thus, ibandronate used orally, possibly represents a promising therapeutic option in the treatment of PDB.
MATERIALS AND METHODS
We studied 12 patients with PDB who were treated with oral ibandronate 150mg monthly for 6 months. Paget’s disease of bone was defined according to established criteria for diagnosis with radiography and bone resorption markers (CTX and AP). Using radiography, the information on location and extent of disease and presence of fractures and lytic lesions were obtained. The common clinical feature in all patients in the study was bone pain. Criteria for therapeutic response, were defined by normal levels of biochemical markers (sAP and sCTX) and clinical improvement after treatment.
The pain was defined as the same, better or worse than in the period before the initiation of treatment. We evaluated the following data: gender (male or female), age (years), bone pain (described as present or absent and compared before and after treatment); sites involved (monostotic or polyostotic); previous treatment with bisphosphonates for more than 12 months (yes or no), serum alkaline phosphatase (sAP), serum C-telopeptide (sCTX) and serum levels of 25OHD.
Serum AP was measured by dry chemical colorimetric method using the VITROS 250/950 (Johnson & Johnson) device with reference values: 38-126U/l. Serum beta-CTX was measured by electrochemiluminescence assay (Elecsys, Roche Diagnostics) with the lower limit of detection of 10pg/ml. With normal reference value: 50-450pg/ml. The methodology for determination of 25OHD was competitive chemiluminescent immunoassay (Liaison, DiaSorin).
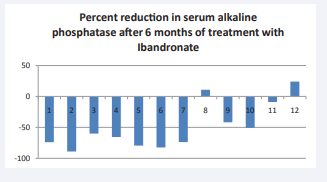
Figure 1: Percent reduction in serum alkaline phosphatase after 6 months of treatment with ibandronate.
Ibandronate 150 mg was administered after fasting for 8 hours with 1 glass of water, under supervision, at the metobolic, ward of Agamenom Magalhães Hospital, monthly for 6 months.
All patients received 1000mg supplemental calcium and 800IU vitamin D per day during treatment with ibandronate. The visits were performed monthly, at the time of administration of medication, individually and at the end of treatment. Clinical examination and evaluation of medication side effects were obtained through notes in the medical records. Exclusion criteria were as follows: inability to maintain upright posture or sitting for 30 minutes, report of chronic use of glucocorticoids, clinically important dysphagia, gastroesophageal reflux disease, severe renal insufficiency, uncorrected hypocalcemia, decompensated hyperthyroidism or hypothyroidism, hypoparathyroidism or hyperparathyroidism, evidence of some other type of bone disease such as osteomalacia or osteogenesis imperfect.
In the data analysis, descriptive statistical techniques were used through statistical measures: mean, standard deviation and percentiles 25, 50 and 75 and inferential statistical technique by paired Student’s t-test. The statistical error used in the statistical tests was 5.0%. The software used for data entry and retrieval of statistical calculations was SPSS (Statistical Package for Social Sciences) version 15.
RESULTS
We studied 12 patients, 7 men and 5 women, with a mean age of mean age 68.6 ± 11,2 years-old (44 to 84). Polyostotic involvement was seen in 9 of the patients studied (75%), the pelvis being the most affected site, present in 58.3% of patients, 41.6% had involvement of the skull and spine and 33.3% of the Femur. Hearing loss was reported at the beginning of the study in 16.6% of the participants, 2 patients had a history of orthopedic surgery and 4 patients had been previously treated with bisphosphonates. Among patients with previous treatment, 2 used Zolendronic acid, 1 used Alendronate and the other Pamidronate, and they were all without medication for more than 12 months, when they began using oral ibandronate. The main baseline parameters are described in Table (1).
Table 1: Baseline chacteristics of the study patients.
|
Table 1: Baseline chacteristics of the study patients. |
|
|
Gender |
7 men: 5 Woman |
|
Age(years) |
68.6 ± 11.2 (44to 84). |
|
Poliostotic/monostotic |
9 (75%)/3 (25%) |
|
sAP(ULN) |
1.49 ± 0.98 (0.55-4.11) |
|
sCTX(pg/mL) |
272.64 ± 176.91 (10-545) |
|
25-OHD (ng/mL) |
36.18 ± 10.90 (26-63.7) |
|
Abbreviations: sAP: Serum Alkaline Phosphatase; ULNx: times the upper limit of normal; sCTX: Serum C-telopeptide; Serum 25-OHD: 25 hidroxivitamin D |
|
The mean reduction of sAP was 49,21 ± 37,9%49.2%. Serum AP was above normal in 7 patients, with an average elevation of 1.5 ± 0.97 times the upper limit of normal (ULN). All patients presented normal sAP after 6 months of treatment.
The mean reduction in sCTX was 65,24 ± 28,9%. In seven patients sCTX was reduced in more than 80% (figure 2).

Figure 2 Serum CTX before and after 6 months of treatment with Ibandronate
The largest reduction was observed in the subgroup that did not make prior use of bisphosphonate, 75.5% ± 25.9%, while the subgroup with prior use of bisphosphonate reduced 44.7% ± 25.7%. Only one patient in the subgroup of patients without previous use of bisphosphonates, had normal sCTX prior to treatment, who showed with a reduction of 97.5% after 6 months of ibandronate, with the largest percentage reduction among all 12 patients in the study.
Serum levels of 25(OH)D were 36.2 mg/dl ± 10.9 with values above 30mg/dl in 9 Patients. Pain was a presenting symptom of the disease in all patients, and at the end of treatment, the proportion of patients with bone pain attributed to PDB decreased significantly, with all patients reporting clinical improvement, being asymptomatic at the end of treatment.
There were no reports of adverse events that could lead to major disruption in the administration of drugs with discontinuation of treatment.
DISCUSSION
Our study showed that oral ibandronate at a dose of 150mg/ month for 6 months was safe and effective for the treatment of PDB. As observed in other studies using oral bisphosphonates in the treatment of PDB, our study showed a higher percentage of sAP normalization with 100% of patients having normal levels after treatment. In one study, oral alendronate at a dose of 40 mg/day for 6 months provides normalization of sAP in only 48% [24].
Siris et al in a study of 162 patients using risedronate, 30mg/ day, during 2 months observed normalization of sAP in 33% of patients and clinical improvement with 42% [15]. In contrast, 30 patients treated with intravenous pamidronate, 30mg/week for 6 weeks achieved normalization of sAP in 53% [30].
Regarding zoledronic acid the mean reduction and normalization of sAP we’re obteined in 96% and 88.6% of patients, reespectivaly [24]. The mean reduction in sCTX obtained in our study, after 6 months of ibandronate, was 65.24%, with reduction in the levels in all patients studied and normalization in 75%. Similar data was observed in the use of oral ibandronate for the treatment of women with osteoporosis. The MOBILE study (Monthly Oral IBandronate In LadiEs) showed a reduction in sCTX of 75.8% after 1 year and 67.7% after 2 years [30].
CONCLUSION
Our data demonstrates high efficacy of oral ibandronate in the treatment of PDB at equivalent doses used in the treatment of osteoporosis.








































































































































