Classifications of Broken Bones
- 1. Head of the Department of Orthopedics and Traumatology, Hospital Universitario “Dr. Jose E. Gonzalez”, Mexico
Abstract
Over time, attempts have been made to unify the way of communicating between orthopedists, without the need to directly see the patient’s image studies or clinical presentation, as well as to create a way to define etiology, treatment or talk about the prognosis according to the type of fracture. Classification systems emerged from this need and although there are inter-observer differences, these are useful tools which will be unified in the following review.
Keywords
Fractures; Classification; Anatomical; Surgical; AO.
CITATION
Peña Martinez VM (2017) Classifications of Broken Bones. JSM Bone and Joint Dis 1(1): 1004.
ABBREVIATIONS
AO: Arbeitsgemeinschaft für Osteosynthesefragen (German for “Association for the Study of Internal Fixation”, or AO
INTRODUCTION
A fracture is definedas a disruption in the continuity of the bone and cover a large spectrum of possible situations, from an undisplaced stress fracture of metatarasal to an open multisegmentary humerus fracture with nervous involment [1].
Even in the earliest written surviving medical text, the Edwin Smith Papyrus, there was a rudimentary classification of fractures. That served to characterize the fracture and to guide the treatment; these are two goals of modern classification systems as well [2].
All systems of fracture classification have served numerous purposes: To characterize fractures according to certain general and specific features, to guide fracture treatment, and to predict outcomes of fracture care [3].
The classification of fractures can be described in terms of characteristics [4]
• Aetiology: Cause
• Morphology: Fracture pattern
• Severity: Involvment of soft tissue or a joint
• Location: Part of the bone affected
• Displacement: Relation between fragments of bone
Etiology:
• Traumatic: Result of forces applied to the bone by a direct/indirect mechanism
• Pathological: Result of a low energy mechanism in an abnormal/diseased bone
• Insufficiency: Result of a low energy in a bone with a decreased mineral density
• Fatigue: Result of cicilical forces with excesive frequency [5].
Morphology:
• Transverse: 30° by a direct force applied to the bone
• Spiral: By an indirect rotational force
• Multisegmentary: Defined as a presence of 3 or more segments of bone
• Avulsion: Caused by traction of ligament, tendon or capsular insertion
• Impaction: When bone fails in axial compression
Severity:
• Open fractures: See Table 1
|
Table 1: Gustilo & Anderson Clasification for Open Fractures. |
||||
|
Fracture Type |
Wound |
Contamination |
Soft-tissue Damage |
Others |
|
I |
<1cm |
Minimal |
Mild |
|
|
II |
>1cm |
Modarate |
Moderate |
|
|
IIIA |
|
Substancial |
Severe |
Coverage adequate |
|
IIIB |
|
Substancial |
Severe |
Coverage inadequate |
|
IIIC |
|
|
|
Arterial injury requiring repair |
• Intraarticular: the fracture disrupts the articular surface.
• Comminution: A high-energy injury and associated with musculoskeletal damage
• Joint dislocation: Loss of contact between the articular surfaces
Location:
• Depends of the anatomical region affected in the skeleton (See Figure 1 & 2)
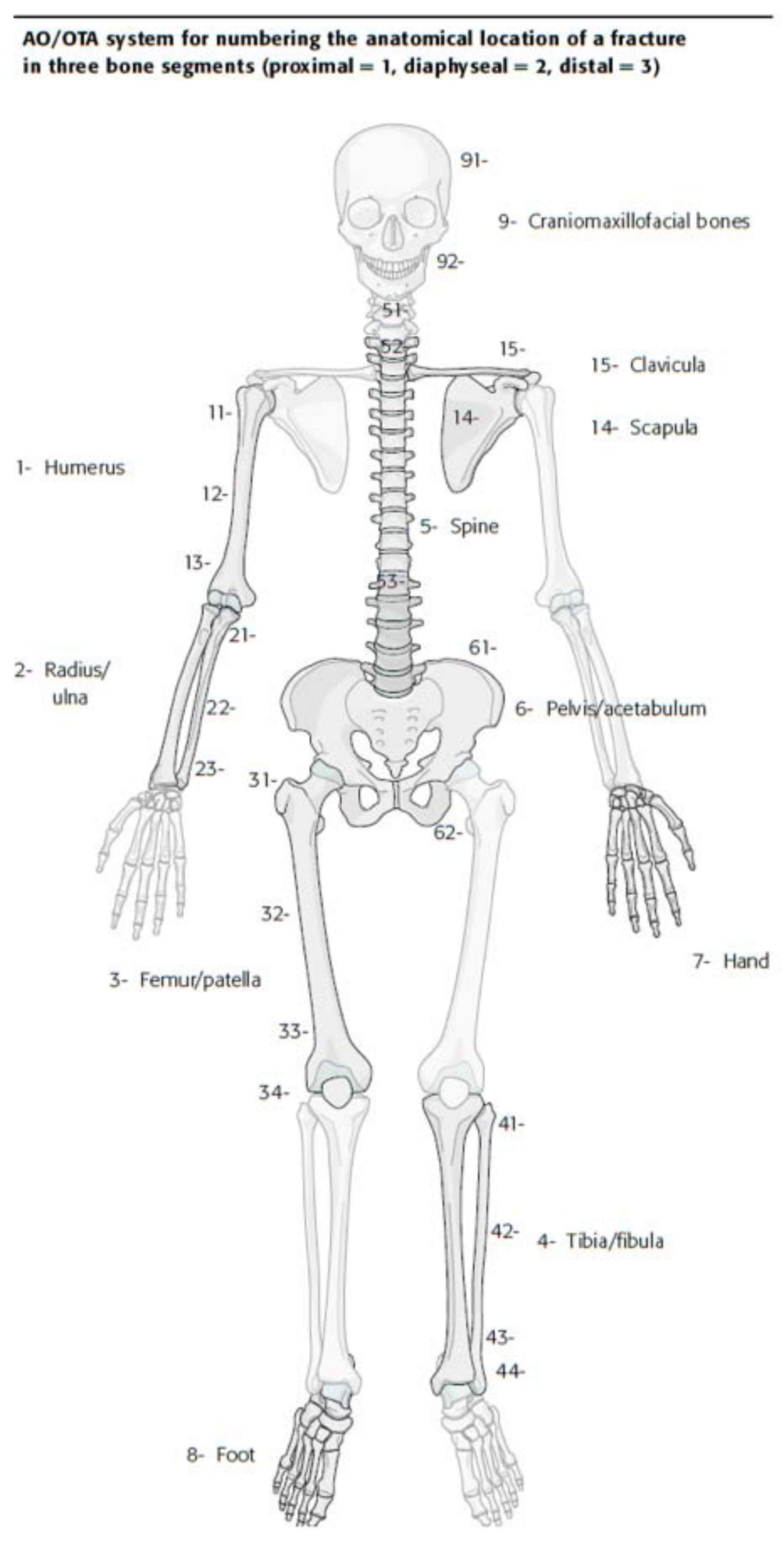
Figure 1: Numeric system for the anatomic location of fracture in three bone segments.
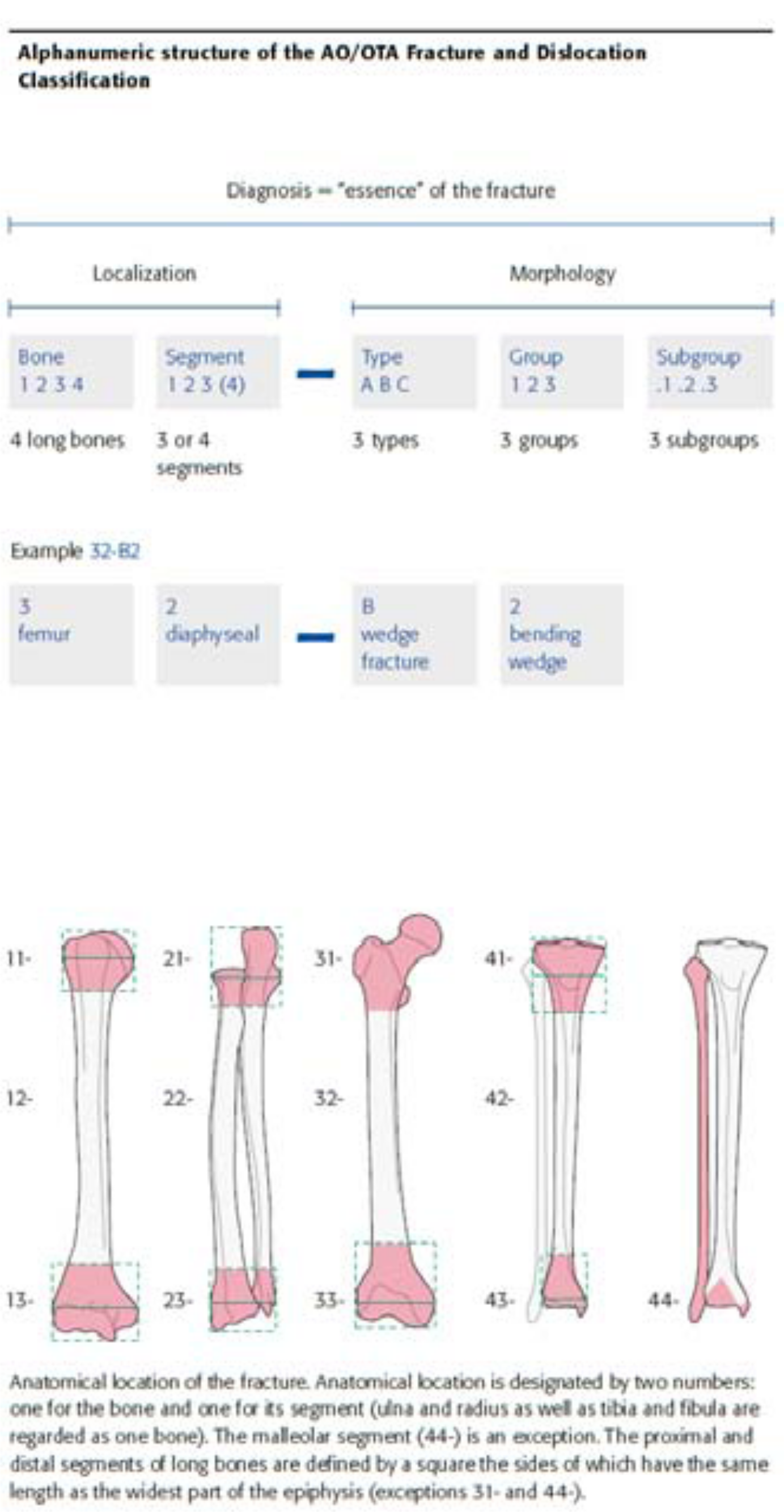
Figure 2: Alphanumeric clasification for bones (AO Clasification).
Displacement:
• Undisplaced: In anatomical position
• Length: Distraction/shortening
• Angulation: Varus/valgus (coronal plane) flexion/ extension (sagital plane)
• Rotation: Internal/external rotation
• Translation: Movement anterior/posterior or /medially/ laterally [6-9]
There are a lot of classifications that could be listed in this review, but it only shows the most prevalent used in our country. Some of the most commonly used fractures classifications of daily clinical practice in orthopedic surgery are described below.
Distal radius fractures
Frykman (1967) the main criteria for classification is the involvement of radiocarpal and radio cubital joint surfaces. There are four groups with two types of fractures each, depending on whether or not ulnar involvement. Its advantages are simplicity and allow reliable conclusions about the prognosis in relation to the cost and the duration of the treatment. As disadvantages: it does not evaluate comminution, it does not reflect the displacement or palmar of the fragments.
Thoracolumbar fractures
The classification system described here exists in order to provide surgeons from different institutions with a common language to discuss various injuries. It provides consistency in injury diagnosis and treatment. The AO Spine thoracolumbar fracture classification system aims to achieve international acceptance.
Type C injuries are segmental injuries. They involve an interruption or separation of both the anterior and posterior components of the vertebral segments. The disruption of the anterior component may be through the disk or vertebral body. The disruption of the posterior elements may be through the spinous process, lamina, pars interarticularis, or posterior ligamentous complex. Type B determines if there is a tension band injury to the spinal column. The presence of a vertebral body fracture can be seen in B and C type injuries. Type A fractures are injuries without posterior wall injury.
Ankle fractures
Niel Lauge-Hansen develop an ankle fracture classification based on foot position at the time of the traumatic event (supination or pronation) and the direction of the deforming forces (abduction, adduction, or external rotation).
Lauge-Hansen created four categories and 13 subgroups of ankle fractures based on his study.
Hip fractures
According to the Tronzo classification system, fractures of types I and II are considered stable while the unstable are the types III, variant, IV and V. Instability criteria of trochanteric fractures included reverse obliquity, posteromedial comminution and sub-trochanteric extending.
CONCLUSION
Fracture classification systems are highly useful for describing patterns; this has been one of the best uses for systems. Using a well-known fracture classification to describe a fracture to an orthopedist or colleague who cannot immediately view the fracture radiographs should bring about in the orthopedist a visual image of the fracture. That enhances communication between orthopedic physicians.
Fracture classification systems are also useful as educational tools.









































































































































{kind=link}