A Patient with Very Unusual Massive Weight Gain from Chronic High Dose NSAID Therapy-Case Report
- 1. Department of Cardiology/Medicine, West Midlands Deanery, UK
- 2. Stafford Hospital, UK
Abstract
NSAIDs do cause weight gain by mechanisms of fluid and water retention. Can chronic high dose NSAID therapy cause massive weight gain? We describe a case of a 69 year old Caucasian lady who was known to have Dercums Syndrome (A rare disorder of painful lipomas). She presented to cardiology out patients via her primary care physician with a history of palpitations and breathlessness over the last few years with no history of syncope, chest pain or dizziness.
She was being treated with high dose Ibuprofen 600mg three times a day for the last 6years!In this duration she gradually gained lot of weight and started developing cardiovascular symptoms. Her symptoms resolved completely following discontinuation of Ibuprofen. In the process of gradually withdrawing her from high dose NSAIDS over weeks she lost nearly 9.2 kg body weight.
Learning objectives: Drugs should be prescribed to patients with lot of care and full understanding of potential side effects and interactions of side effects with patient characteristics.
Full drug history is pertinent in approaching any case as it is often overlooked. In this case, it shows how important drug history is to manage this patient’s symptoms. This could in fact save a lot of resources from doing unnecessary investigations trying to look for causes of her symptoms. Medication review should be done at every earliest opportunity to avoid adverse effects. This patient was on high dose of Ibuprofen for the last 6years and she could be at risk of other serious side effects involving kidneys, liver, gastrointestinal tract. Chronic high dose NSAID therapy could lead to alarming weight gain with fluid and salt retention causing cardiovascular side effects.
Keywords
Weight gain; NSAIDs; Ibuprofen; Dercums syndrome
Citation
Mohammed I, Ibrahim N, Alsoud M (2013) A Patient with Very Unusual Massive Weight Gain from Chronic High Dose NSAID Therapy-Case Report. JSM Clin Case Rep 1(1): 1006.
INTRODUCTION
We have decided to write up this interesting case for sharing as there are a few learning points that we can benefit from.
Firstly, majority of patients with Dercums syndrome are characterised by painful lipomas and lot of non specific symptoms too. In this case, the lady presented with shortness of breath and peripheral oedema, therefore this lady was suspected to be having major cardiovascular problem and was referred to
cardiology out-patient department.
Secondly, we all as doctors have been trained to collect a comprehensive drug history for every patient including prescribed medications, over-the-counter medications, herbal remedies and any illicit drug use. Using this case for example, Non-steroidal anti inflammatory drug (NSAID) was the main culprit for her symptoms. If the drug history was not looked into thoroughly, we could be missing out on the most important aspect of this case presentation.
Last but not least, the interesting fact is, since stopping her NSAID (amidst the fact that she was quite on a high dose of Ibuprofen which she has been taking daily for the last 6years), her symptoms completely resolved.
CASE PRESENTATION
We describe a 69 year old Caucasian lady who has worked as a nurse. She was seen in cardiology clinic with complaints of shortness of breath, palpitations and increase in weight over the last few years. Symptoms were gradually worsening over few years and she started to get some swelling on her feet. And these symptoms were significantly affecting her day to day quality of life. There was no history of chest pain, dizziness or syncope. She was otherwise normally fit and well. She denied any history of psychiatric problems or compulsive water drinking. Her appetite was normal for good no of years. Past medical history includes Dercums syndrome, hypothyroidism and pernicious anaemia.
There was no family history of kidney problems or Dercums syndrome. Drug history included Levothyroxine 100mcgs OD, HRT, Cyanocobalamin colecalciferol high dose, Ibuprofen 600mg TDS for last 6 years. She was allergic to Penicillin. She was a nonsmoker and occasionally drinking alcohol in small quantities. Clinical examination revealed bilateral pitting leg oedema upto the knees. Jugular Venous Pressure was normal. Weight recorded was 67 kg with height of 163 cm.Pulse was 76bpm regular and normal volume.Blood pressure recorded was 136/78 mm Hg Cardiovascular system examination was normal as also was examination of other systems.
This patient’s symptoms gradually developed over years with progressive shortness of breath, mild oedema on the legs, palpitations on exertion and few episodes of light headedness. She also gained weight but never recorded serial measurements of her weight. Her symptoms initially suggested those of congestive heart failure and fluid build up. Her echocardiogram showed good biventricular function and no significant valvular disease or chamber enlargement. There was no heart rhythm abnormality detected on 24 hr holter monitoring. Investigations like, full blood count, thyroid function tests, serum cortisol and renal function tests were normal. Other tests like liver function tests, serum osmolarity were normal. There was no evidence of proteinuria or casts in urine and urine osmolality was normal. She was advised to wean off NSAID treatment by substituting her pain control with codeine and paracetamol.She gradually lost weight of 9.2kg after stopping NSAIDs and also gradually all her symptoms disappeared completely. We concluded that the patient’s symptoms and presentation were from pathological
effects of chronic high dose NSAID therapy causing fluid and water retention and abnormal weight gain.
DISCUSSION
NSAIDs can cause sodium and water retention and have been found to be harmful in patients with compromised cardiovascular conditions and also in patients with renal disease [1].This patient demonstrated sodium and water retention resulting in enormous weight gain to the extent of feeling short of breath, experiencing palpitations on regular basis and also feeling dizzy at times. These symptoms can be explained by increase in plasma volume and
physiological increase in cardiac output due to active sodium and water retention. As recommended in British National Formulary (BNF), the dose of Ibuprofen can be increased to a maximum of 2.4g daily if necessary, however maintenance dose of 0.6g- 1.2g daily may be adequate. This patient was on 1.8g daily for the past 6years as maintenance (high dose) and it is an interesting fact that the side effects of the medication were giving her weight gain and symptoms.
Mechanisms by which NSAIDs cause sodium and water retention are shown in (Figure 1).
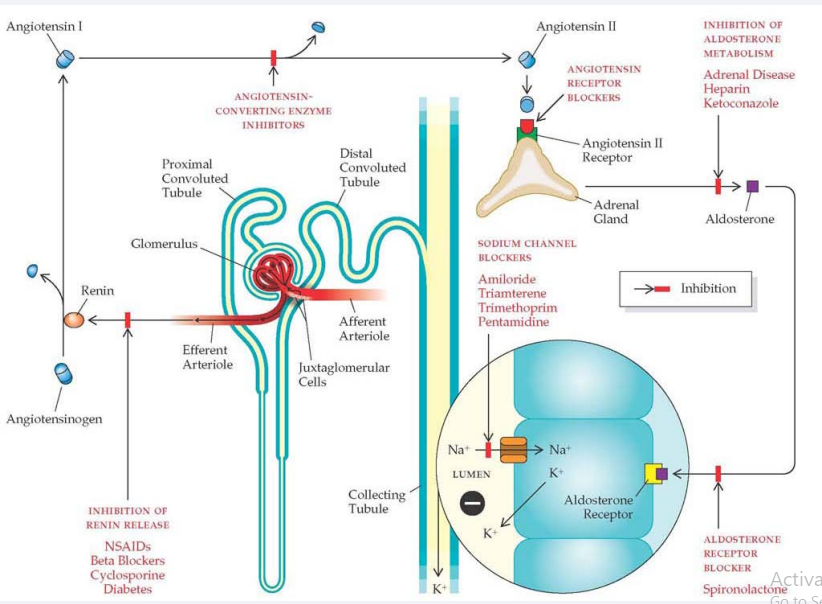
Figure 1 Showing various sites where NSAIDs can act on of human nephron.
It’s a well known fact that NSAIDs have cardio renal effects in patients. Prostaglandins modulate the functions of ion and water transport at the level of renal tubules. Of importance are two prostacyclins PGE2 and PGI2.The PGE2 is responsible for the regulation of sodium reabsorption in the renal tubule [2].Non-steroidal antiinflammatory drugs (NSAIDs)inhibit the cyclo-oxygenase(COX) enzymes thus reducing the prostaglandins production [3].This in turn results in changes in modulation of kidney function [4]. In particular PGE2 inhibition leads to increased sodium reabsorption resulting in fluid retention and peripheral edema. Although described as one of the mild side effects, of NSAIDs, this can result in weight gain of 1-2 kg within 1st week of therapy [1]. This can have deleterious effects in patients with established heart failure [2].Our case had immense weight gain resulting from chronic high dose NSAID therapy.NSAIDs have also been recognised to cause membranous nephropathy, interstitial nephritis and minimal change disease [5]. Nawaz et al described a case of relationship between recurrent nephritic syndrome with use of NSAIDs which was proved with renal biopsy showing deposits of abundant IgG1,weak IgG4 and positive staining for phospholipase A2 receptor [5].The extent of NSAIDs effects on the kidney depends on the premorbid condition of the kidney. Patients who have a longstanding chronic renal failure will be more vulnerable to the effects compared to patients with healthy kidneys [3]..However in our case there was no evidence of renal impairment and all the physiological effects of fluid and salt retention causing weight gain completely resolved after withdrawal of NSAID therapy. In some studies there is some evidence of subclinical renal dysfunction in patients with long term NSAID therapy by evidence of reduced creatinine clearance and impaired urine concentrating ability [3].
With the new selective NSAIDs specifically inhibiting either COX-1 or COX-2 enzymes, some researchers argue either one is better than another with renal side effects.However,new data suggests both COX-1 and COX-2 enzymes are involved in prostaglandin synthesis [4].COX-1 is constitutively expressed in renal vasculature,glomerular mesangial cells and both cortical and medullary portions of the collecting duct [1,6-8]. Meanwhile, COX-2 is predominantly expressed intraglomerularly in podocytes and at low levels in macula densa.
The expression of COX-2 in the renal cortex is up regulated in response to decreased sodium intake, volume depletion, renal artery stenosis, active lupus nephritis, partial renal ablation and therapy with inhibitors of the rennin-angiotensin system [9]. In the medulla, however COX-2 expression is inversely proportional to the salt content in the circulating volume [10].The pattern of COX-2 expression in the kidney highlights their importance in regulating water and electrolyte homeostasis.
Patient’s clinical examination and cardiovascular investigations were normal. There was no pathological reason found for her profound weight gain and also for her unintentional weight loss apart from the reason being her chronic high dose Ibuprofen. She was completely well and symptom free with normal weight 6 months after stopping Ibuprofen!
INVESTIGATIONS
Patients with abnormal weight gain need full battery of investigations to rule out pathological causes of weight gain. Focus should be mainly on cardiovascular, renal and endocrine mechanisms.
1. Electrocardiogram (ECG): sinus rhythm with a rate of 72 beats per minute with no ischemic changes and all parameters were within normal limits.
2. Echocardiogram: Good biventricular function with normal chambers and valves except mild mitral and mild tricuspid regurgitation.
3. 24 hour tape normal sinus rhythm
4. The routine blood tests full blood count, renal parameters, eGFR, liver function tests and thyroid function tests were within normal limits.
5. Patient had urine examination, urine osmolality and serum osmolarity examination and also an ultrasound examination of kidneys was undertaken which was normal.









































































































































{kind=link}