An Unusual case of Osteopetrorickets presenting as Neonatal Hypocalcemic Seizures and Dilated Cardiomyopathy
- 1. Pediatric Endocrinology, B J Wadia Hospital for Children, Mumbai, Maharashtra
Citation
Shreya S (2021) An Unusual case of Osteopetro-rickets presenting as Neonatal Hypocalcemic Seizures and Dilated Cardiomyopathy. JSM Clin Case Rep 9(1): 1184.
Abstract
Background: Osteopetrosis is a rare genetic condition of reduced osteoclastic bone resorption. Excessive calcium sequestration in bone may lead to an abnormal Ca/P balance resulting in hypocalcemia and poor mineralization of the osteoid ( rickets).
Case Characteristics: We report the case of a one month old boy with late onset neonatal hypocalcemia and rickets that was later diagnosed as Osteopetro-rickets.
Message: Osteopetrosis should be kept in mind as a rare cause of neonatal hypocalcemia and rickets.
INTRODUCTION
A 1 month old boy presented with hypocalcemic seizures and dilated cardiomyopathy. He was diagnosed as malignant autosomal recessive form of infantile osteopetrosis at 4 months of age due to presence of anemia, hepatosplenomegaly, failure to thrive, visual and hearing loss, and the typical radiological images on plain radiograms. His medical history revealed third degree consanguineous parents and one brother’s death at 40 days of life of unknown etiology (similar symptoms). The patient had associated clinical and laboratory findings of superimposed rickets on osteopetrosis. Osteopetrosis should be borne in mind as a rare cause of neonatal hypocalcemia and rickets.
CASE REPORT
A 1-month-old boy was referred to our center in view of multiple hypocalcemic seizures and cardiogenic shock due to dilated cardiomyopathy. Serum calcium was low at 6.7 mg/dl (normal, 8.0-11 .5 mg/dl), with serum phosphorus of 3.8 mg/ dl (normal, 3.5-6.0 mg/dl), alkaline phosphatase of 1214 U/L, with an appropriately elevated level of iPTH of 466 pg/ml and low Vitamin D levels ( 25-OHD =10.6 ng/ml ). Serum sodium, potassium, magnesium, bicarbonate, urine pH and urine calcium/ creatinine ratio were normal and associated renal tubular acidosis was excluded.
2-D Echo revealed poor contractility with poor ejection fraction of 30 %. Infant initially received intravenous calcium gluconate and transiently required inotropic agents to augment cardiac contractility. He simultaneously received a mega-dose of Vitamin D (1.5 lakh U) intramuscularly. He was then started on short term oral Calcitriol (0.5 microgram/day) along with oral calcium supplementation at 100 mg/kg/day.
He was born of third degree consanguineous marriage, at term, by normal vaginal delivery without complications and his birth weight was 3500 grams. Family history was significant in form of previous male offspring having abnormally large head, and multiple seizures in the neonatal period, with death occurring on day 40 of life.
At 5 months of age, infant was noted to have clinical features of active rickets, in the form of frontal bossing, depressed nasal bridge, wide open anterior fontanelle, widening of wrists, prominence of the costochondral junction, and pectus carinatum. Infant was severely growth retarted with anthropometric parameters below the -3SD except head circumference, which was between 1 to 2 SD. Skeletal survey (figure 2) revealed marked sclerosis and cortical thickening predominantly within the skull (figure 3) base with typical “space alien” face.
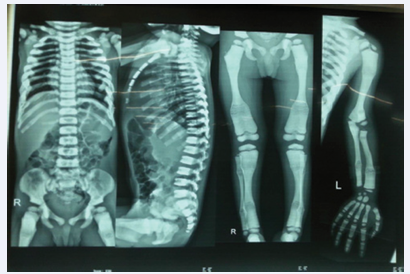
Figure 2 Skeletal Survey of child.
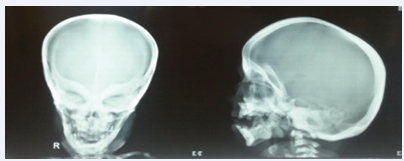
Figure 3 Skeletal X-ray of child characterize.
There was diffuse bony sclerosis and bone-within-bone appearance involving the long bones, radiolucent and radio-opaque bands with the thoracolumbar spine showing characteristic sandwich vertebrae. Metaphyseal fraying and cupping of bones of knee joint was noted on the patient’s radiographs (figure 1).

Figure 1 Lower limb of radiograph display.
These findings, along with the lowered serum levels of calcium and phosphorus, were consistent with superimposed rickets on osteopetrosis
Hematological complication included normocytic normochromic anemia with a hemoglobin level of 8.1 g/dl (normal, 10.5-13.5 g/dl) and hematocrit of 26% (normal, 33- 39%). The WBC and platelet counts were normal.
Incidentally, ophthalmologic examination revealed cataract in both eyes for which child was subsequently operated at 3 years of age. Brainstem Auditory Evoked Potential revealed mild sensorineural hearing loss in left ear. At subsequent follow up, child was noted to have nystagmus in both eyes and visualevoked potentials revealed bilateral optic neuropathy. His other issues were delayed dentition, poor growth velocity and global developmental delay. Cranial imaging was not done due to cost constraints. He suffered from obstructive sleep apnea due to persistent nasal stuffiness. There were no fractures during the follow up of 6 years.
The patient continues to receive symptomatic and supportive treatment including rhino pharyngeal disinfection, calcium and vitamin D supplementation. Patient was advised for bone marrow transplantation which was not possible due to logistic issues and cost constraints.
DISCUSSION
Osteopetrosis is a rare hereditary bone disease characterized by osteoclast dysfunction and an abnormal accumulation of osseous tissue. It encompasses a group of highly heterogeneous conditions, ranging in severity from asymptomatic to fatal in infancy. The more severe forms tend to have autosomal recessive inheritance, while the mildest forms are observed in adults and are inherited in an autosomal dominant manne [1]. Four clinical forms are recognized-the infantile malignant autosomal recessive form (ARO), the intermediate autosomal recessive form, autosomal recessive form with renal tubular acidosis and the adult benign autosomal dominant form [2].
Malignant infantile osteopetrosis (MIOP) is the autosomal recessively inherited form of this disease that generally begins in utero, and presents at birth [3], or within the first year of life. It has an incidence of 1 in 2,50,000 births [4].
Osteopetro-rickets is a rare association of osteopetrosis with rickets that has been elucidated in various case reports [5,6]. Kaplan et al reported a series of five infants with osteopetrosis, all of whom had proven cases of rickets [7] Although it is a state of intense positive balance of body calcium, the skeleton sequesters more than 99% of the calcium, so that the serum level of calcium paradoxically may decrease. The calcium phosphorus product becomes <40, thus insufficient for mineralization. In such cases, there is chance for hypocalcemic tetany or seizures. [3] This association is considered a paradox in the midst of plenty.
The increased bone mass can result in phenotypic features such as macrocephaly and altered craniofacial morphology including choanal stenosis. Tooth eruption defects and severe dental caries are also common. The longitudinal growth of bones is impaired, resulting in short stature of varying degrees. The neurological manifestations of osteopetrosis are secondary to obstruction of the foramina through which the cranial nerves, spinal cord and major blood vessels transverse the skull, resulting in blindness, hearing loss, facial palsy, and hydrocephalus [8]. The most severe complication of ARO is bone marrow suppression. The abnormal expansion of bone interferes with medullary hematopoiesis, resulting in life-threatening pancytopenia, and secondary expansion of extramedullary hematopoiesis sites such as the liver and spleen.
At present, no effective medical treatment for osteopetrosis exists except for symptomatic treatment. Treatment of rickets with calcitriol (1,25-hydroxyvitamin D3) and high levels of dietary calcium decreases the prevalence of lethargy, irritability, poor feeding and upper respiratory tract infection in these patients. Presence of rickets has additional implications if hematopoietic stem cell transplantation is anticipated [2,7], When normal bone is replaced by hypo mineralized osteoid(rickets), the effectiveness of transplantation is severely attenuated. Because normal osteoclasts cannot resorb hypo mineralized osteoid , rickets counteracts the basic purpose of the transplantation [7]. Therefore, one of the principal objectives of the radiographic evaluation of these patients before transplantation is to search for underlying rickets so that it can be eradicated before bone marrow transplantation.
REFERENCES
1. Stark Z, Savarirayan R. Osteopetrosis. Orphanet J Rare Dis. 2009.
2. Balsan S, Garabédian M. Rickets, osteomalacia, and osteopetrosis. Curr Opin Rheumatol. 1991;3: 496–502.
3. Engiz O, Kara S, Bagrul D, Lahr G, Alioglu B, Arikan I, et al. Infantile malignant osteopetrosis: a rare cause of neonatal hypocalcemia. J Pediatr Endocrinol Metab. 2012; 25: 1205–1207.
4. Loría-Cortés R, Quesada-Calvo E, Cordero-Chaverri C. Osteopetrosis in children: a report of 26 cases. J Pediatr. 1977. ;91: 43–47.
5. Olgaç A, Tümer L, Boyuna?a Ö, K?z?lkaya M, Hasano?lu A. Diagnostic dilemma: osteopetrosis with superimposed rickets causing neonatal hypocalcemia. J Trop Pediatr. 2015; 61: 146–150.
6. Datta V, Prajapati NC, Kamble M, Pathak S. Osteopetrorickets. Indian Pediatr. 2000; 37: 98–99.
7. Kaplan FS, August CS, Fallon MD, Gannon F, Haddad JG. Osteopetrorickets. The paradox of plenty. Pathophysiology and treatment. Clin Orthop Relat Res. 1993; 294: 64–78.
8. Al-Tamimi YZ, Tyagi AK, Chumas PD, Crimmins DW. Patients with autosomal-recessive osteopetrosis presenting with hydrocephalus and hindbrain posterior fossa crowding. J Neurosurg Pediatr. 2008; 1: 103–106.









































































































































{kind=link}