Cauliflower Ears and Saddle Nose in Relapsing Polychondritis- Clinical Image
- 1. Rheumatology Department, Limerick University Hospital, Limerick, Ireland
Citation
Mohamed Ashraf FA, Mhuircheartaigh ON, Anjum S, Fraser A (2014) Cauliflower Ears and Saddle Nose in Relapsing Polychondritis- Clinical Image. JSM Clin Case Rep 2(1): 1019.
CLINICAL IMAGE
A 46-year-old Caucasian lady with a background history of previous bilateral uveitis presented with progressive shortness of breath and increase exercise tolerance. She was noted to have nasal dorsal concavity, shortened vertical nasal length and bilateral auricular damage but denied any history of previous trauma. Few years before she developed symmetrical active synovitis of the small joints of her hands and feet however no diagnosis was confirmed at the time and over the space of four months the inflammation self-resolved. Physical examination revealed “saddle” deformity of her nose (Figure 1), bilateral “cauliflower” ears (Figure 2), tenderness to palpation over her anterior trachea and wheeze.
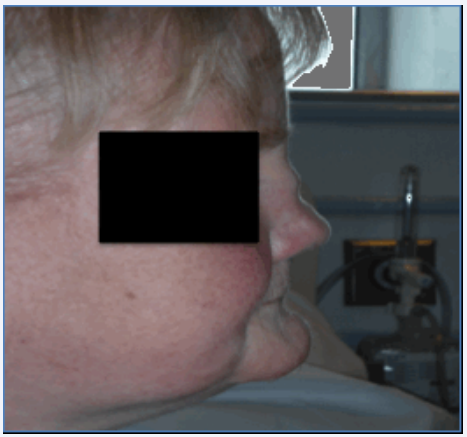
Figure 1 Showing “saddle” deformity of the nose due to chondromalacia and collapse of her nasal septum.

Figure 2 Showing “cauliflower” ear caused by recurrent chondritis and structural alteration of the auricles with the sparing of the non-cartilaginous lobule.
Worsening of her dyspnoea and development of stridor led to tracheostomy placement.
Computed tomography (CT) of the neck and thorax revealed a subglottic stenosis and bronchial stricture. Her erythrocyte sedimentation rate (ESR) was 100 mm/hr. Serology revealed a negative rheumatoid factor (RF), anti cyclic citrullinated peptide (anti-CCP), antinuclear antibodies (ANA), and anti-neutrophil cytoplasmic antibody (ANCA). Her skin testing for tuberculosis and serological testing for syphilis were negative. Based on her clinical features, a diagnosis of relapsing polychondritis was made and she was commenced on systemic corticosteroid therapy and concomitant escalating dose of oral methotrexate (10mg weeklyinitially, which were then increased to 15mg weekly) where her condition significantly improved.
Relapsing polychondritis is a rare connective tissue disease characterized by episodic inflammation and eventual destruction of cartilaginous tissues, with characteristic clinical findings [1]. The most common presenting features include recurrent pain, swelling and redness of the external ear [1,2] and nose resulting pinna deformity or “cauliflower” ears and “saddle” deformity of the nasal bridge [3]. However other signs and symptoms could occur including ocular, airways, joints, cardiovascular, cutaneous and central nervous system involvement. Patients presenting with this clinical features should aware the physician regarding the possible diagnosis of relapsing polychondritis.









































































































































{kind=link}