Complete Stress Fracture of Both Forearm Bones
- 1. SISLI HAMIDIYE ETFAL EAH, ISTANBUL, TURKEY
Abstract
Stress fracture in non-weight bearing bones is uncommon. Complete stress fracture of both forearm bones without overt risk factors is a very rare condition. This report presents the case of a 68-year-old female patient with displaced stress fracture of both bones of forearm. The fractures were treated with open reduction and plate fixation. To our knowledge this is the first case in the literature presenting with complete stress fracture of both forearm bones in the absence of intrinsic risk factors. Awareness of stress fractures of forearm may prevent displacement and progression to complete fractures.
Keywords
Forearm; Stress fracture; Radius; Ulna
Citation
BasriSezer H, Talmac MA, Armagan R,TugrulEren O (2016) Complete Stress Fracture of Both Forearm Bones. JSM Clin Case Rep 4(1): 1096.
ABBREVIATIONS
CRP: C - Reactive Protein; DEXA: Dual Energy x-ray Absorptiometry
INTRODUCTION
Stress fracture is incomplete or complete fracture of bones due to repetitive loads in magnitudes less than required for an acute fracture. Stress fractures are generally found in weight bearing bones of athletes and very rarely seen in non-weight bearing bones. Ulna is the most commonly affected long bone in the upper extremity [1].
Stress fractures of ulna have been reported due to a variety of sport activities (Polo, tennis, kendo, weight lifting, break dance etc.) and use of crutches in elderly [2,3]. The location of fracture is diaphysial in young athletes and torsional loads are responsible for the fracture. In elderly, fractures are located mostly in the proximal third of ulna due to compressive and distractive loads.
There is a variety of risk factors for stress fractures. They can be categorized as intrinsic and extrinsic. Factors affecting the durability and flexibility of bone are intrinsic risk factors such as bone mineral density, bone turnover rate, alignment and composition of the body hormonal factors and nutritional factors. Extrinsic risk factors include mechanical factors that increases loads on bones such as sport activities.
This report presents the case of a 68-year-old female patient with stress fracture of both bones of forearm which occured during nursing of her crippled husband. To the best of our knowledge, this is the first case in the literature with complete stress fracture of both forearm bones
CASE PRESENTATION
A 68-year-old female patient admitted to our out-patient clinic with left forearm pain existing for six months. The pain was insidious onset and started after she began nursing of her husband who was unable of self care and mobilization after a cerebrovascular insult. She admitted to a clinic with the same complaint and she was evaluated with x-rays which revealed no bony pathology and given a conservative treatment of oral and topical antiinflammatory medications and bandages for soft tissue pain. She reported that the pain continued to increase and her functions gradually became worse as she has taken care of her husband. When she admitted to our clinic the pain was not relieved with oral analgesics and worse for the last one week and her functions were limited due to pain. The patient was normal looking with a normal body mass index (20,5). On examination the left forearm was deformed and edematous. Palpation revealed pain and crepitus in the middle third of the forearm. The x-ray examination revealed fracture of both radius and ulna diaphysis and fragmentation of ulna in the distal third (Figure 1).

Figure 1 Preoperative X-ray image.
Computerised tomography (Figure 2), magnetic resonance image of the left forearm (Figure 3) and scintigraphic examination were carried out.
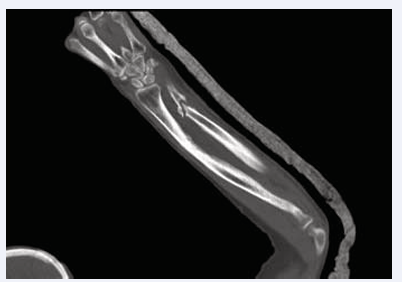
Figure 2 Preoperative computerized tomography image.

Figure 3 Preoperative magnetic resonance image.
Scintigraphy supported our diagnosis of stress fracture. MRI revealed bone edema beside the fractured forearm and noticed about the osteomyelitis in the differential diagnosis. There was no lytic bone lesion or mass detected. A detailed blood test was carried out including blood sedimentation rate, CRP and parathormone. There was no hormonal imbalance or increase in the acute phase reactants. DEXA values of the patient was also in normal limits.
The patient was treated with open reduction and plate fixation for both bones. The closed medullary canal was opened in both ulna and radius. The defect in the ulna was 1 cm and filled with autologous spongious graft obtained from iliac crest. The patient was allowed to perform early passive motion of her hand and elbow but advised to protect her arm from loads for 6 weeks. She began to use her left hand after 6 weeks.
In the last follow up in the 12 months, there was no pain and complete functional recovery (Figure 4).
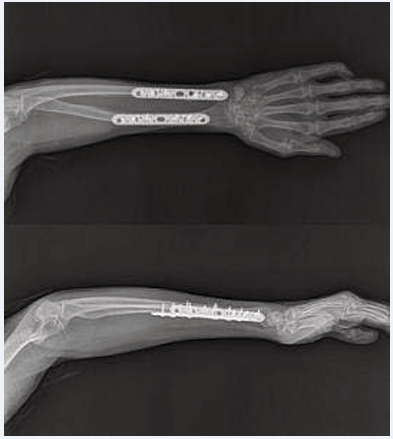
Figure 4 Postoperative x-ray image at 12 months follow-up.
DISCUSSION
Stress fracture of the forearm may be due to repetitive traction, compression or torsional forces. There may be underlying risk factors affecting the bone quality or increasing the loads applied. The case presented in this report is otherwise normal in body structure and there was no intrinsic risk factor like osteoporosis or medications like biphosphonates. She was not performing a professional sport or activity other than nursing her husband.
Our case is unique in the literature because stress fracture of forearm usually present with ulnar pain and displaced cases were usually ulna fractures. To our knowledge this is the first case in the literature presenting with displaced fracture of both forearm bones with no obvious underlying intrinsic risk factor.
]Early radiographic examination may reveal normal results in stress fractures. Therefore awareness and clinical suspicion may be the critical point in the diagnosis of the stress fractures and prevention of the displacement. If there is no displacement nonoperative treatment with casts may be used for treatment [2].
In case of displaced fractures x-ray examination may be enough to detect fracture and may show callus formation around the fractured region. To make a definitive diagnosis MRI, bone scintigraphy may also be helpful. Computerized tomography may show bone defects as in our case which may be critical to plan the operation.
Displaced forearm fractures must be treated with anatomical reduction and internal fixation as if they are intraarticular fractures.
CONFLICT OF INTEREST
The authors declare that there are no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.









































































































































{kind=link}