Intrapulmonary Cystic Teratoma of Lung
- 1. Department of Pulmonology, SVS Medical College and Hospital, India
Abstract
Teratomas are benign germ cell tumors that are usually found in the gonads.
Citation
Nithin Kumar Reddy R, Lavanya A, Waghray P (2022) Intrapulmonary Cystic Teratoma of Lung. JSM Clin Case Rep 10(2): 1200
INTRODUCTION
They have low malignant transformation potency [1,2,3]. Extra-gonadal germ cell tumors are considered rare. Mediastinum is the most common site of extragonadal germ cell tumor [4] but can also arise in other areas such as the head and neck [5], retroperitoneum, sacrococcygeal region and on rare occasions the lung, which is considered as an intrapulmonary teratoma (IPT) [6]. Teratomas are composed of one or multiple tissues such as hair, sebaceous glands. Teeth and other tissues derived from germ cells. Microscopically, it is composed of endodermal, ectodermal, mesodermal components. Pancreatic tissue, mucinous epithelium, respiratory epithelium, epidermal tissue with sebaceous glands, adipose tissue smooth muscle, and cartilage can be identified.
CASE PRESENTATION
A 18-year-old male presented to OPD with complaints of cough, shortness of breath, chest discomfort for two weeks. Cough was mainly non-productive in nature with no postural or diurnal variation. Shortness of breath was insidious in onset, gradually progressed from grade 0 MMRC to grade 2 MMRC in duration of two weeks. Patient gives a history of low-grade fever one episode two weeks back.
On examination, Pulse rate 90/min, BP 110/70 mm Hg, Temperature - 1000F, Respiratory rate - 18/min, SpO2 96%@ room air. Breath sounds are decreased in lower 2/3rd of Right Lung.
Chest X-Ray
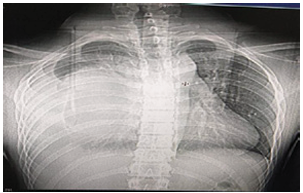
Chest X- Ray examination reveals Homogenous opacity in Right Middle and Lower Zone with Tracheal and mediastinal shift towards Left side without obliteration of Costo Phrenic angle.
A Diagnostic Pleural aspiration was attempted in outside Hospital as the Chest X-Ray showing Homogenous opacity in Right Hemi thorax which had a possible differential diagnosis of Right sided massive Pleural effusion. USG chest performed which showed cystic consistency with hypo and hyper echoic foci with air bronchogram. Later CT Chest was performed which revealed
the following findings.
CT Chest
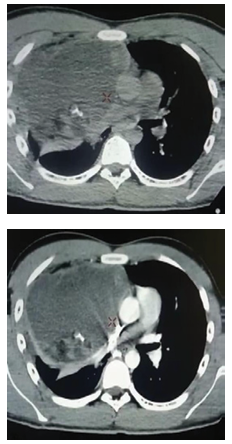
Pre and Post Contrast Helical CT acquisition of Chest done on MDCT scanner reveals large well circumscribed heterogeneously enhancing mixed density mass lesion (CC 152 x ap 126 x 125mm) with foci calcifications/ fat attenuation and septations seen in anterior mediastinal region compressing the right upper, middle and lower lobes and Anterior mediastinal tumor possibly Teratoma. Patient was referred to cardiothoracic surgery department for Surgical Management and Excision.
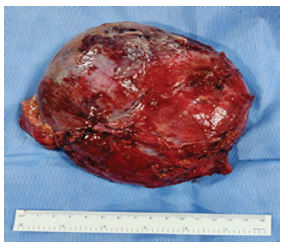
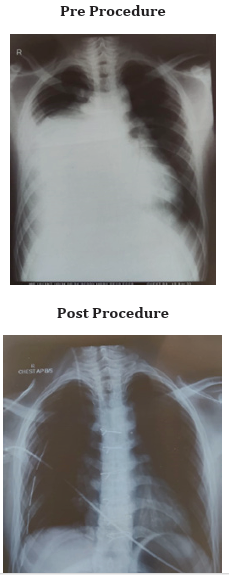
A 15x15cm thick fleshy mass with thick sebaceous material was seen intraoperatively and intercostal drainage tube was put. Post-operative period was uneventful. Patient was discharged after three days.
DISCUSSION
The age presentation is wide, but the typical presentation in adults is in first and second decades of life. The presenting
symptoms for IPTs are variable. Most common are chest pain, hemoptysis, and cough but these are all common symptoms making preoperative diagnosis difficult. Trichoptysis - is an extremely rare symptom [7], whereby patients cough up hair. It is highly specific for rupture of mediastinal teratoma into tracheobronchial tree. The Wide variety of symptoms by which this condition presents makes the clinical diagnosis of IPT [8,9] extremely difficult and hence mainly reliant on radiological investigations. The evidence provided by CT scan is invaluable and serves two important purposes. Firstly, CT assists in making the diagnosis [10] of this rare tumor with clinically indistinguishable characteristics. Secondly, CT determines whether the tumor has ruptured or not. Differential diagnoses of anterior mediastinal mass include-Thymoma, Thymic carcinoma, Thymic lipoma, Thymic cyst, Hodgkins lymphoma, Non-Hodgkins lymphoma, Germ cell tumors/Teratoma, Thyroid/Sub sternal Goitre.
CONCLUSION
In this Case report, we present a rare case of a benign intrapulmonary teratoma in an 18 year-old male involving the Right Middle and Lower mediastinum of the lung. Every homogenous opacity in lung fields are not pleural effusions, other potential causes of anterior mediastinal masses like teratoma should be kept in mind to make accurate diagnosis.
REFERENCES
- Giunchi F, Segura JJ. Primary malignant teratoma of lung: report of a case and review of the literature. Int J Surg Pathol. 2012; 20: 523-527.
- Choi JS, Bae YC, Lee JW, Kang GB. Dermoid cysts: epidemiology and diagnostic approach based on clinical experiences. Arch Plast Surg. 2018; 45: 512.
- Bal A, Mohan H, Singh SB, Sehgal A. Malignant transformation in mature cystic teratoma of the ovary: report of five cases and review of the literature. Arch Gynecol Obstet. 2007; 275: 179-182.
- Yalagachin GH. Anterior mediastinal teratoma-a case report with review of literature. Indian J Surg. 2013; 75: 182-184.
- Lack EE. Extragonadal germ cell tumors of the head and neck region: review of 16 cases. Hum Pathol. 1985; 16: 56-64.
- Gatcombe HG, Assikis V, Kooby D, Johnstone PA. Primary retroperitoneal teratomas: a review of the literature. J Surg Oncol. 2004; 86: 107-13.
- Abhishek Chandrakant Sawant, Ajay Kandra, Swapna Reddy Narra. Intrapulmonary cystic teratoma mimicking malignant pulmonary neoplasm. BMJ Case Rep. 2012; 2012: bcr0220125770.
- Schlumberger HG. Teratoma of the anterior mediastinum in the group of military age; a study of 16 cases, and a review of theories of genesis. Arch Pathol (Chic). 1946; 41: 398–444.
- Ali MY, Wong PK. Intrapulmonary teratoma. Thorax. 1964; 19: 228–35.
- Morgan DE, Sanders C, McElvein RB, et al. Intrapulmonary teratoma: a case report and review of the literature. J Thorac Imaging. 1992; 7: 70–7.









































































































































{kind=link}