Lisinopril Induced Angioedema
- 1. Department of Internal Medicine, University of Florida, USA
- 2. Department Internal Medicine, Semnan University of Medical Sciences, Iran
Citation
Khurram T, Arezo F, Fauzia R (2014) Lisinopril Induced Angioedema. JSM Clin Case Rep 2(3): 1038.
CLINICAL IMAGE
Angioedema is a non-inflammatory, nonpruritic, localized swelling of the skin that can affect any part of the body but is more frequently recognized on lips, tongue, face, glottis, oropharynx, periorbital, gingival and genital areas and on the extremities [1,2]. Most cases of angioedema are benign however, depending on the location and the underlying structures being compressed, it can lead to severe respiratory complications and even death [3,4]. Release of prostaglandins and histamines are usually implicated in the vasodilation and edema associated with angioedema [5]. While angioedema can be hereditary our current case focuses on medication-induced, acquired angioedema. The list of medications that can cause angioedema can include proton pump inhibitors, statins, certain antibiotics with the beta-lactam ring, nonsteroidal anti-inflammatory drugs (NSAIDS). While ACE inhibitors and angiotensin-receptor blockers (ARBs) are both implicated in the etiology of acquired angioedema, it is the ACE inhibitors (ACE is) that are most often associated with this process [5]. The incidence of ACE is related angioedema is between 0.1-0.7% [6] and although it is a very rare side effect, it has been implicated in respiratory arrest and death [3,7,8]. ACE is consumed by millions of patients throughout the world for their beneficial use in heart failure, hypertension and nephropathy [7,9]. Management is usually symptomatic and may involve the use of subcutaneous epinephrine injections, antihistamines and steroids [5,10]. Severe cases may warrant an admission to the intensive-care units for airway protection and respiratory support (Figure 1).
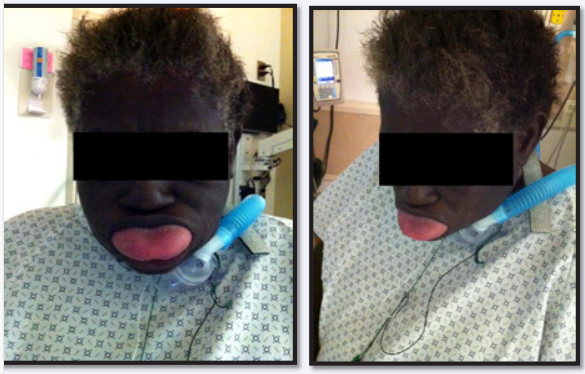
Figure 1 Patient is an elderly female who was recently started on Lisinopril, an ACEi. During her first week, she took the medication twice and developed mild respiratory distress each time. Ironically, non-compliance proved beneficial as the patient did not take her next dose until after a few. On her third dose, she developed a very severe episode of respiratory distress. Fortunately the patient survived owing her life to the tracheostomy procedure.
Our medical picture presents the case of an elderly female patient who was recently started on Lisinopril for management of hypertension. Her first dose resulted in mild swelling of tongue and lips. The swelling soon subsided and the patient did not take another dose over the next few days. This time the swelling of the tongue was worse than the previous episode. The patient still waited at home and did not seek medical attention. She took her third dose the following week which resulted in severe angioedema of the tongue and oropharynx. She was treated with epinephrine, antihistamine, steroids and owes her life to respiratory support through the tracheostomy tube especially in the initial phase of the episode. This can be seen in the medical pictures above.
Our case goes on to signify the onset of life threatening angioedema with the use of ACE is. Special caution should be taken with aggressive patient follow-ups when prescribing ACE is to the elderly or to individuals with limited social network and support as they may resist the urge to seek medical attention which could culminate in severe complications including death.









































































































































{kind=link}