Long Term Outcome of Extraskeletal Ewing
- 1. Department of Orthopedic Surgery, Chang Bing Show Chwan Memorial Hospital, Changhua County, Taiwan
- 2. Department of Radiation Oncology, Taichung Veterans General Hospital, Taichung, Taiwan
Abstract
Extraskeletal Ewing Sarcoma (EES) is a rare type of Ewing’s Sarcoma (ES) that arises in soft tissue with high local recurrence rate and distant metastasis rate. Here we report a case of locally advanced EES of the thigh in a middle-aged male Asian adult diagnosed 15 years ago. It was a local disease initially and the patient underwent limb salvage surgery plus postoperative interstitial brachytherapy and adjuvant chemotherapy as his first treatment. Multiple episodes of lung metastasis over the patient’s left lung were discovered during the first seven years of diagnosis in spite of multiple surgical resections, as well as adjuvant chemotherapy. The disease has been under control for eight years after the last local radiotherapy to the lung metastasis at the lower lobe of left lung (LLL). The patient continued follow up at our outpatient department (OPD) with no local recurrence or distant metastasis being recorded since his last radiotherapy treatment was completed. Our review suggests that interstitial brachytherapy after a wide excision with a free margin may be an alternative treatment for preserving the limb in patients diagnosed with locally advanced soft tissue sarcoma. Although EES has an aggressive disease process, multimodal treatment may help to control the disease progression.
Keywords
Extraskeletal Ewing sarcoma , Interstitial brachytherapy , chemotherapy , long term survival
Citation
Tai-Sheng T, Hao-Wei L, Hui-Ling Y (2021) Long Term Outcome of Extraskeletal Ewing’s Sarcoma of the Thigh after Multimodal Treatment including Limb Salvage Surgery Plus Interstitial Brachytherapy: A Case Report. JSM Clin Case Rep 9(1): 1186.
ABBREVIATIONS
EES: Extraskeletal Ewing Sarcoma; ES: Ewing’s Sarcoma; LLL: Lower Lobe of Left Lung; OPD: Outpatient Department; CT: Computed Tomography; LUL: Left Upper Lung; BED: Biological Effective Dose; EQD2: Equivalent Dose in 2 Gy fractions.
INTRODUCTION
EES is a rare type of ES that arises in soft tissue and commonly affects the paravertebral area, lower extremities, head and neck and pelvis [1]. Since the cells of ES, peripheral primitive neuroectodermal tumors and EES all share the same DNA abnormalities and similar proteins; they are grouped into the same family of malignant tumors and have the same treatment policy. Unlike ES which develops mainly in children and young adults, EES is more likely to occur in patients younger than five years of age or older than 35 years of age [2]. Large tumor size (> 8 cm), high lactate dehydrogenase, metastasis at presentation, poor histological response to chemotherapy, radiotherapy only as local treatment and a positive surgical margin have all been indicated as poor prognosis indexes in a recent report [1]. The prognosis for patients is poor, as most of them die of metastatic disease to the lung or liver within one to two years of initial diagnosis [3]. EES has high local recurrence rate and when the disease arises in a low extremity, amputation of the limb is sometimes unavoidable if the tumor is bulky. Limb salvage surgery, combined with postoperative radiotherapy can preserve the structure and function of the limb. In addition to having a high local recurrence rate, distant metastasis is common in a patient who has been diagnosed with locally advanced EES. Here we report a case of EES of the thigh in a middle-aged Asian male experiencing long term survival after undergoing multimodal treatment involving limb salvage surgery plus postoperative interstitial brachytherapy.
CASE PRESENTATION
A 48-year-old man presented pain and soreness at his right thigh over one week, which he experienced while climbing stairs. The soreness sensation at the middle portion of his right thigh involved tenderness and did not respond to medication for pain control prescribed by his family doctor. Upon physical examination, a round, unmovable smooth-surfaced mass, approximately 10 x 7 cm, was palpable at the middle portion, medial area of the right thigh. Magnetic Resonance Imaging revealed a heterogeneous high-density mass, approximately 7 x 5 cm in size, located between the right rectus femoris and the intermedius muscle on T1-weighted + contrast medium (Figure 1a,1b) and T2- weighted images (Figure 1c,1d).
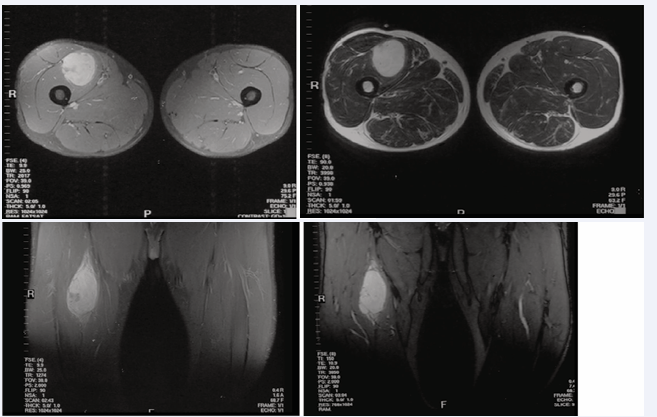
Figure 1 A heterogenous high density mass, approximately 10 x 7 cm in size, located between the right rectus femoris and the intermedius muscle on T1-weighted with contrast medium (a, b) and T2- weighted images (c, d).
A PA chest X-ray showed there were no active lung lesions as well as no abnormal findings from a routine blood test or chemical test, with the exception of high blood sugar levels. A frozen section examination revealed an extraskeletal Ewing’s sarcoma/ primitive neuroectodermal tumor, for which the patient then underwent a wide excision procedure. An intraoperative interstitial brachytherapy catheters implantation was requested by the surgeon due to the possibility of marginal resection of the bulky tumor (Figure 2).
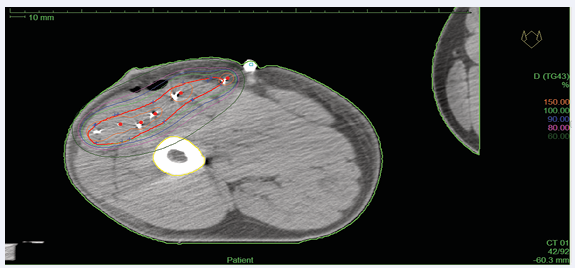
Figure 2 Radiation dose distribution of interstitial brachytherapy to the tumor bed plus a 2 cm margin.
The pathology report showed extraskeletal Ewing’s sarcoma/ primitive neuroectodermal tumor of the thigh with diffuse expressed CD99 and vimentin, focally positive to bcl-2, and negative for CD34, CD117, LCA, AE1/ AE3, EMA, and S-100. The resection margin of the muscle was not involved by the tumor cells. On the 4th day after surgery, the patient received high dose rate interstitial brachytherapy at 400 cGy per fraction, BID, over four days for a total tumor dose of 3200 cGy. The planning target volume was directed to tumor bed plus a 2 cm margin in all directions after avoiding 5 mm of the skin and femoral bone. Chemotherapy with a modified VAIA regimen (Vincristine, Ifosfamide, Mesna, and Adriamycin) for four cycles was then prescribed to him after radiotherapy. Six months after adjuvant chemotherapy, a single small nodule, sized 1.5 x 1.5 cm, was found at the LLL on computed tomography (CT) scan of the chest (Figure 3).
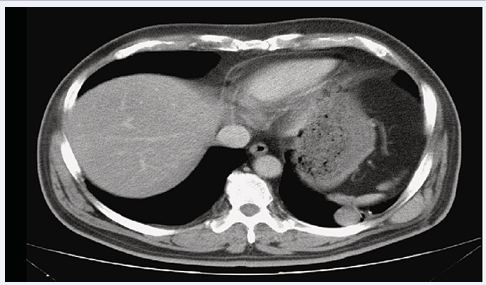
Figure 3 A single small nodule, size 1.5 x 1.5 cm, was found at lower lobe of the left lung on CT scan of the chest one year after the right thigh wide excision.
A subsequent lung wedge resection for tumor removal demonstrated a metastatic Ewing’s sarcoma/ primitive neuroectodermal tumor. The patient was then treated with adjuvant chemotherapy involving a VIP regimen (VP16, Ifosfamide, and Cisplatin) for four cycles. Unfortunately, a metastatic lesion was again found at the LLL from CT scan of the chest three weeks after having finished adjuvant chemotherapy (Figure 4).
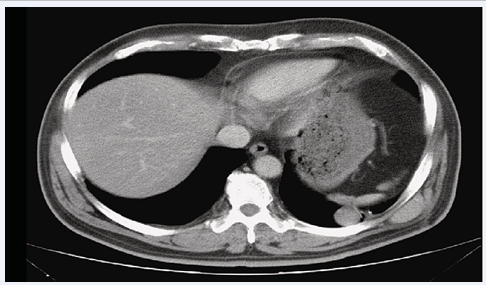
Figure 4 A metastatic lesion was found once again at lower lobe of the left lung on CT scan of the chest two years after the right thigh wide excision.
The patient received another wedge resection for the tumor at the LLL. This time, postoperative radiotherapy was directed to the tumor bed using 6000 cGy in 30 fractions, which was delivered smoothly after surgery. However, a newly developed nodule (2.3 cm x 1.4 cm) located next to the left subclavian artery was discovered during a routine check-up which had included a CT scan of the chest during OPD follow-up (Figure 5).
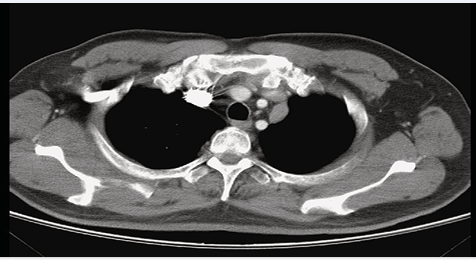
Figure 5 A newly developed a nodule (2.3 cm x 1.4cm) next to the left subclavian artery was found from during a routine check- up involving a CT scan of the chest during an OPD follow-up three years after the right thigh wide excision.
A thoracoscopic wedge resection of the tumor at the left upper lung (LUL) was performed. A metastatic extraskeletal Ewing’s sarcoma/ primitive neuroectodermal tumor was proved through histological examination of the resected tissue. A bulging mass which had grown progressively at the left lower back was noted ten months after the second operation on the lung, and proved to be a metastatic extraskeletal Ewing’s sarcoma. Five months after the resection of the chest wall tumor, a tumor nodule sized 2.5 cm was found at LUL on CT scan of the chest. Another thoracoscopic wedge resection of the LUL lung for the removal of the tumor was performed and a metastatic extraskeletal Ewing’s sarcoma/ primitive neuroectodermal tumor was proved again upon histologic examination. The patient then received six cycles of chemotherapy with CyVDIC (cyclophosphamide, vincristine, and dacarbazine) at our Hematology Department. Re-assessment after chemotherapy via CT scan of the chest showed that a nodule sized 4 x 4 cm had progressively enlarged once again in the left upper mediastinum, abutting on the left brachiocephalic vein and left subclavian artery. The image of the tumor was in favor of local recurrence once again. Since there was high risk of left subclavian artery injury during surgery, no additional surgical resection was planned. The treatment policy was then shifted to local radiotherapy, with a total radiation dose of 6000 cGy in 30 fractions being prescribed to the tumor at the left upper lung field. This time, the tumor at the upper mediastinum regressed well after radiotherapy (Figure 6).
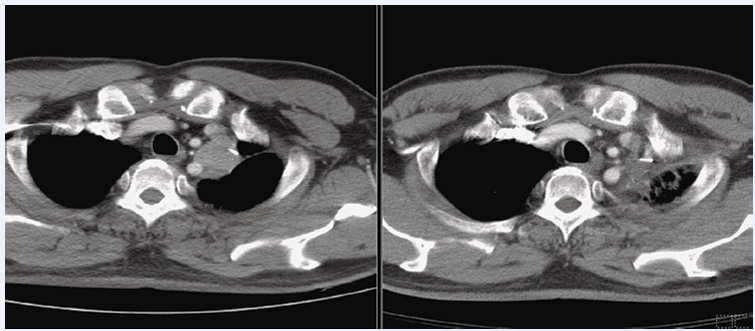
Figure 6 A nodule recurrent, size 4 x 4 cm, enlarged progressively in the left upper mediastinum, abutting on the left brachiocephalic vein and left subclavian artery seven years after the right thigh wide excision (A); The recurrent tumor at the upper mediastinum regressed well after radiotherapy eight years after the right thigh wide excision (B).
There was no additional surgical management or chemotherapy planned for the patient due to his poor general condition after experiencing many rounds of multi-modal treatments. Over the course of eight years of followup after the patient’s final radiotherapy treatment, there was no local recurrence of tumor found at the right thigh or any sign of distant metastasis at the lung or elsewhere.
DISCUSSION
The radiosensitivity of Ewing sarcoma was first recognized by James Ewing in 1921 [4]. And in the past, surgery and radiation therapy were the only known treatment methods for ES, with the long term survival rate being less than 10% prior to the identification of chemotherapy response in the 1960s [5]. The introduction of multi-agent chemotherapy increased both the local control rate and survival rate in 1970s. Currently, multimodal treatment has now become a common practice in the treatment of Ewing’s family sarcoma. Both surgery and postoperative radiotherapy improve local control of Ewing sarcoma on the extremities alone. The recommended radiation doses range from 45 to 60Gy, with radiotherapy local control varying from 53 to 86% [6]. The radiation dose for definitive radiotherapy is in the range of 55 to 60 Gy, while the radiation dose for postoperative gross tumor is at least 55.8Gy, with the radiation dose required for microscopic tumor being 45Gy [6]. Interstitial brachytherapy delivers high doses of radiation directly to the tumor bed without compromising the regional normal organ and is therefore an option for delivering high dose radiation to the tumor bed at the extremities after a wide excision of the tumor. The biological effective dose (BED) and equivalent dose in 2 Gy fractions (EQD2) for our patient using interstitial brachytherapy for a total tumor dose of 32 Gy in 8 fractions, BID, was 42.24 Gy and 35.2 Gy. The response of our patient was good and there was no local recurrence during 15-years follow up period. Multimodal treatment which improves patient clinical outcomes has been reported [2,3]. Patients with EES have been treated using rhabdomyosarcoma chemotherapy protocols in the past, but now they are being treated with the same chemotherapy protocol for ES [7]. The addition of ifosfamide and etoposide to a standard regimen does not affect the outcome for patients with metastatic disease, but it does significantly improve the outcome for patients with either nonmetastatic Ewing’s sarcoma, primitive neuroectodermal tumor of the bone, or primitive sarcoma of bone, as was reported in an earlier clinical trial [6]. The same results were also seen in our patient when he suffered from multiple left lung metastases. Fortunately, the patient’s disease response well to his last local radiotherapy, and no more metastatic lesions were found at his left upper lung or anterior upper mediastinum or elsewhere during clinical follow in the following eight years.
It is rare to find an EES in middle-aged Asian men. Although EES has an aggressive disease process, multi-modality treatment may help to control the disease progression.
ACKNOWLEDGEMENTS
This study was supported by Taichung Veterans General Hospital.









































































































































{kind=link}