Malignant Transformation of Omental Endometriosis Presenting With Neurological Manifestations
- 1. Department of Obstetrics and Gynaecology, JIPMER, Puducherry, India
- 2. Department of Obstetrics and Gynaecology, JIPMER, Puducherry, India
- 3. Department of Obstetrics and Gynaecology, JIPMER, Puducherry, India
- 4. Department of Obstetrics and Gynaecology, JIPMER, Puducherry, India
- 5. Department of Pathology, Puducherry, India
Abstract
Background: Adenosarcoma of endometriosis presenting with neurological paraneoplastic manifestations is rare. Case: 30 year old multiparous woman presented to neurologist with stroke. Subsequent evaluation revealed haemorrhagic ascites with adnexal masses and pulmonary thrombosis. Her CA 125 level was very high and ascetic fluid cytology showed adenocarcinoma deposits and she was treated as advanced ovarian malignancy. The plan was to give neoadjuvant chemotherapy and do interval debulking after treating pulmonary thrombosis with anticoagulants. She developed haemorrhagic ascites and pleural effusion and desaturation while on anticoagulants immediately after first cycle of chemotherapy and was managed for the same. Laparotomy after stabilisation revealed large multiple friable tumor masses in the peritoneal cavity, Omentum and rectovaginal septum. Uterus and adnexa appeared normal. Evacuation of freely floating tumor masses, resection of rectovaginal and omental masses and TAH with BSO with infracolic omentectomy was carried out. Histopathological examination showed transition of benign endometriotic elements and malignant stromal component with sarcomatous changes in tumor masses fulfilling the Sampson’s and Scott’s criteria for malignant transformation of extrauterine endometriosis. Chemotherapy was restarted (paclitaxel and carboplatin) after surgery and was given for 3 cycles. But she developed recurrence in pelvic lymphnodes and parametrium after 3 cycles. She was later treated with Ifosphamide for which she reponded with disappearence of recurrence. Literature search did not reveal a similar case presentation and this may be the first case of adenosarcoma of omental endometriosis presenting with neurological manifestations.
Cite this article
Dasari P, Manikandan K, Sagili H, Raju AA, Verma SK (2013) Malignant Transformation of Omental Endometriosis Presenting With Neurological Manifestations. JSM Clin Case Rep 1(1): 1010.
ABBREVIATIONS
CT: Computerised Tomography; MTP: Medical termination of Pregnancy; LMP: Last menstrual period; FFP: Fresh Frozen Plasma
INTRODUCTION
The possibility of malignant transformation in endometriosis was first described by Sampson in 1925 [1]. Malignant transformation of endometriosis is rare and adenosarcomam is one of the very rare malignancies reported to occur in preexisting endometriosis [2]. Adenosarcomas can occur in uterine and extrauterine sites. A large recent review reported 24 cases of adenosarcomas in extrauetrine endometriosis [3]. Coagulation disorders and concurrent systemic thrombosis are common in cancer patients and may result due to malignancy itself inciting a low grade coagulopathy or due to chemotherapy or Radiotherapy [4]. A case of primary peritoneal adenosarcoma arising in extrauterine endometriosis who presented clinically with neurological symptoms due to cerebral thrombosis is reported here due to its rare clinical presentation and difficulties in diagnosis.
CASE PRESENTATION
A 30 year old multiparous lady presented to Neurology Outpatient department with right hemipaeresis and slurring of speech of 4 days duration. There was no history of fever, headache, seizures or vomiting. She gave history of distension of abdomen of 10 days duration. Neurological examination showed right upper motor nerve facial paralysis and right hemiparesis. Computerised Tomography (CT) brain done outside showed a small granulomatous lesion in left sylvian fissure. It was thought to be due to thrombosis and she was advised to take tab asprin 150 mg and tab atorvastatin 20 mg and to undergo Electrocardiogram (ECG), 2 D Echocardiogram (ECHO) and Ultrasonogram ( USG) of pelvis and abdomen. USG abdomen showed an adnexal mass with free fluid in the abdomen and hence she was advised Gynaecology consultation.
Gynaecological evaluation revealed that she was para 1 and underwent a first trimester MTP (Medical termination of pregnancy) 7 months back elsewhere. Her present menstrual cycles were regular and she suffered from stroke on the 2 nd day of her LMP (Last menstrual period). She noticed abdominal distension 10 days ago and bowel and bladder habits were normal.
On examination, she was moderately built and nourished, had mild palor and tachycardia. She was normotensive and her thyroid was normal. Abdomen was mildly distended with free fluid and there was some vague reisistence without any definite palpable mass. Per speculum examination showed healthy cervix and vagina and on per vaginal examination size of the uterus was not made out. There was forniceal bulge and no nodules or mass could be appreciated. On per rectal examination, rectal mucosa was smooth and no mass was felt. Ultrasound examination of abdomen and pelvis showed a large complex adnexal mass posterosuperior to uterus with free fluid. Diagnostic aspiration of the free fluid revealed haemorrhagic ascites. A provisional clinical diagnosis of ovarian malignancy was made and she was hospitalized and investigated further
Her haemogram , Liver function tests , renal function test,
ECG and X-Ray chest and Upper GI (gastrointestinal) endoscopy were normal. PT- 19.6, INR 1.64. CA 125 was 2323.8 IU/L and other tumor markers were within normal limits. Four days after admission she recovered completely from her stroke. Repeat CT brain was normal but CECT abdomen Pelvis and thorax showed pulmonary saddle thrombus extending in to main segmental branches along with ascites and bilateral ovarian masses and omental thickening (Figure 1 A&B).
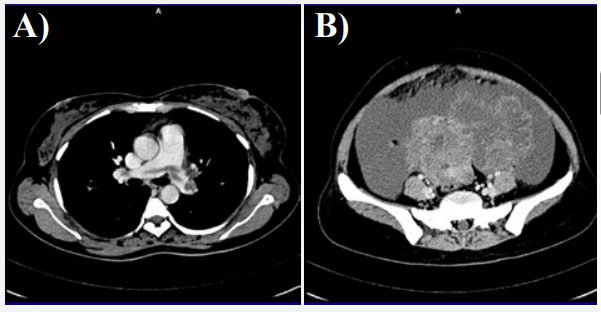
Figure 1 A: CT Thorax showing pulmonary saddle thrombosis. B: Ascites with omental thickening and bilateral masses interpreted as from Ovaries.
Doppler study showed normal IVC (Inferior vena cava) and bilateral compressible popliteal veins. ECHO heart was normal.
Physcian, Cardiothoracic Surgeon and Cardiologists opinions were sought regarding pulmonary thrombus and she was started on anticoagulants (Heparin and Warfarin).
Ascitic fluid cytology was reported as adenocarcinoma deposits. It was planned to give neoadjuant chemotherapy and do interval ldebulking surgery after discussion in tumor board. She was started on the first cycle of chemotherapy employing Carboplatin, Paclitaxel and she developed sudden onset dyspnoea and increased abdominal distension and decreased oxygen saturation on the second day of chemotherapy (Day 18 of anticoagulation). Her X-ray chest showed right sided pleural effusion and her INR on this day was >4. Anticoagulants were stopped and she was given protamin sulphate , vitamin K, 8 FFP ( fresh frozen Plasma), 3 packed cell transfusion and was managed in intensive care unit with ventilator support for 2 days. Her tachypnoea setteled after slow abdominal decompression by draining one litre of ascitic fluid. After normalization of INR, her investigations were repeated. ECHO was normal and there was no pericardial or pleural effusion and no evidence of thrombus. She was taken up for laparotomy after 12 days of the above event. There was haemorrhagic ascites of more than 2 litres with few old blood clots and 2 fleshy necrotic tumor masses of more than 10x10 cms lying freely in peritoneal cavity. There was a large solid mass 16 x10 cm with cystic areas attached to the omentum (Figure 2 A&B) and another mass of about the same size in POD attached to the rectovaginal septum.
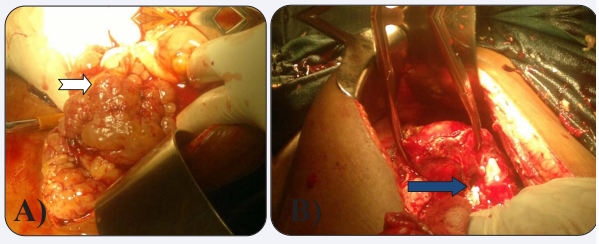
Figure 2 Intraoperative findings. A: Shows the friable mass in the omentum. B: Shows normal uterus and ovaries the arrow points to normal ovary.
Sigmoid colon was adherent to the posterior surface of uterus and broad ligament. Uterus and adnexa appeared normal except for a few minute extrinsic deposits. Ascites was drained and the freely floating tumor masses were removed and the tumor masses attached to the omentum and rectovaginal septum were easily excised. Total abdominal hysterectomy with bilateral salphingoopherectomy and infracolic omentectomy was performed and a drain was kept in POD (Pouch of Douglas). All the other abdominal organs were normal and there were no palpable lymphnodes. Surgical staging was Stage III and the surgical differential diagnosis was Primary= peritoneal carcinoma/Omental malignancy/Metastatic disease.
Post-operatively she received injection Enoxaparin for 7 days and the drain was removed after 4 days and sutures on 10 th day. Her post operative course was smooth. Her CA 125 was 42.5 IU/L and thrombophilia work up for acquired as well as inherited thrombophiliasa was reported to be normal. Repeat ECHO was normal. CE CT (Contrast enhanced Computer Tomography) abdomen, pelvis and thorax after one month of surgery reported
as normal except for a small nodule in the left breast the FNAC of which was fibroadenoma. There was no evidence of residual disease in abdomen and pelvis.
The histopathological report of primary surgery took almost a month and it was as follows: Multiple sections from the masses show lesions composed of epithelial and stromal elements. Epithelial part shows endometrial lining with tubal metaplasia which at places shows mild nuclear atypia and stratification. In some sections there are cystically dilated glands and in some places the glandular component is compressed in to slit like spaces. Few areas show normal appearing endometrial glands with surrounding stroma. The stromal component shows marked overgrowth compared to the glandular component. There is periglandular increased stromal cellularity moderate phleomorphism in some sections and occasssional mitosis. Secondary changes in the form of stromal decidualisation, fibrinous exudates and haemorrhage are also noted. Cervix showed squamous metaplasia and myometrium is normal. The final report is adenosarcoma arising in omental endometriosis with a low grade stromal sarcomatous componenent. Endometriosis involving left ovary with surface invagination by endometriotic foci. Immunohistochemistry was positive for ER, PR, Vementin in glands and stroma; EMA, CK 7 highlighted epithelial component (glands) ; CK 20, CEA, CA 125,CD 10, CD 68 and Desmin were negative (Figure 3).
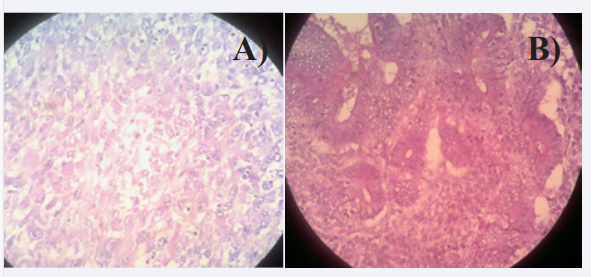
Figure 3 A: Histopathological picture showing adenosarcoma. B: Histopathological picture showing omental endometriosis with the transitional changes of adenosarcoma.
The final diagnosis based on the laparotomy findings and the histopathological report of the masses is primary peritoneal mullerian adenosarcoma which fulfills the Sampson’s and Scott’s criteria [5,6] viz;1. Histological evidence of endometriosis in close proximity to the tumor. 2. No other identifiable site of malignancy 3. Histological appearance of the tumor compatible with an origin in endometriosis and 4. Continuous histological transition of benign endometriosis merging with malignant component.
The patient was re- started on chemotherapy employing Carboplatin and Paclitaxel after discussion with the tumor board and a follow up CECT 3 cycles of chemotherapy showed illdefined focal lesions with small calcific areas of sizes 1.6 x 1.3 cms in right and left parametria respectively (Figure 4) Another 1.2 x1 cm focal lesion was noted in the pelvis on right side adjacent to Psoas muscle.
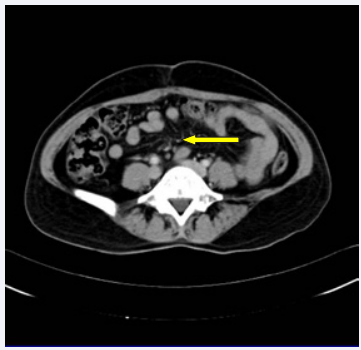
Figure 4 Follow up CT pelvis shows Pelvic lymphadenopathy. Arrow points to enlarged pelvic lymphnode.
Few right common iliac nodes were present, the v largest was 4 mm. Carboplatin and Paclitaxel were stopped and she was treated with 3 cycles of Ifosphamide and the subsequentCT showed resolution of the above metastatic deposits. It is since 3 months after the last dose of chemotherapy and a year after surgery the patient is alive and gained weight and leading a normal life.
DISCUSSION
Neurological paraneoplastic syndromes occur in less than 1% of patients with cancer. Cerebrovascular complications in cancer patients may be due to thrombosis, infarction or haemorrhage and stroke or coma may be the only clinical presentation sometimes. Recognition of these unusual stroke syndromes can lead to identification of occult and treatable cancer or the presentation may also be due to advanced malignancy [4]. A retrospective cohort study found the risk of stroke to be 1.44 fold higher in young patients with head and neck cancers when compared to stroke in non-cancer individuals [7]. The present case was asymptomatic until she had neurological symptoms due to stroke due to thrombosis though her malignancy was advanced. The clinical, radiological findings of abdomen and pelvis were those of ovarian malignancy and the diagnosis was supported by a highly elevated tumor marker i. e. , CA 125. Of the gynaecological malignancies ovarian tumors are the common cause of paraneoplastic manifestations. All these lead to a preoperative diagnosis of advanced ovarian malignancy.
A pre-operative diagnosis of endometriosis was not thought of in this case as the woman was multiparous and the clinical findings were not typical of endometriosis. Endometriosis presenting with haemohagic ascites is rare and is reported in literature [8,9] Malignant transformation of endometriosis is reported to occur in 10.8 % of cases and the commonest site of malignancy is ovarian endometriosis (5%) [10]. Malignant transformation of extrauterine endometriosis occurs in 1% of the cases [10,11]. And the types of malignancies that occur in] endometriosis were classified in to 3 groups viz 1. Epithelial ovarian cancers (endometrioid adenocarcinoma and clear cell carcinoma), 2. Other Müllerian-type tumors, including Mülleriantype mucinous borderline tumor and serous borderline tumor and 3. Sarcomas such as adenosarcoma and endometrial stromal sarcoma [2]. The present case was diagnosed to be extrauterine adenosarcoma. Adenosarcomas occur most commonly in uterine endometrium followed by ovary. Rare and unusual sites include the peritoneum, intestine, vagina, urinary bladder, liver, and round ligament. A case of concurrent adenomyosis, and ovarian, omental, colonic and lymph nodal endometriosis intimately associated with the adenosarcoma demonstrating the transition was reported by Liu W and Axiotis CA [3]. They reviewed the literature between 1977 and 2008 and found 24 cases fulfilling the histological criteria. Primary peritoneal mullerian adenosarcoma with sarcomatous overgrowth associated with endometriosis was reported by Dincer and collegues [11]. Their findings were similar to the present case in that there were multiple tumor masses lying free in the pelvic cavity and subdiaphrgmatic spaces. Omental masses similar to the present case were also found in the case reported by Liu W and Axiotis CA. Masses in the rectovaginal septum were reported by\ Raffaelli R and collegues [12]. The present case did not respond to chemotherapy employing paclitaxel and carboplatin and the tumor activity is noted to be progressing. This is evident by the fact that the CECT of abdomen, pelvis and thorax performed after surgery were normal. But after 3 cycles of continuation of neoadjuvant chemotherapy lymphnodal metastasis was found. Adenosarcoma recurs [12] and can metastasize to lymphnodes [3] as reported by others and also evidenced in the present case.
Literature review revealed that this is the second case of primary peritoneal mullerian adenosarcoma arising in endometriosis and the transition is obvious on histopathological examination. This may be the first case of adenosarcoma arising in extrauterine endometriosis presenting with neurological manifestations as our literature search did not find any other case presenting with neurological manifestations
ACKNOWLEDGEMENTS
Dr. Rakhee Kar, Assistant Professor, Department of Pathology, for her assistance in histopathological diagnosis.
REFERENCES
2. Higashiura Y, Kajihara H, Shigetomi H, Kobayashi H. Identification of multiple pathways involved in the malignant transformation of endometriosis (Review). Oncol Lett. 2012; 4: 3-9.
3. Liu W, Axiotis CA. The relationship between primary extrauterine adenosarcoma and the secondary mullerian system.: Report of a unique case demonstrating histologic transition between benign and malignant elements and a review of literature. N A J Med Sci. 2010; 3: 132-135
4. Rogers LR. Cerebrovascular complications in cancer patients. Neurol Clin. 2003; 21: 167-192.
5. Sampson JA. Endometrial carcinoma of the ovary arising in endometrial tissue in that organ. Arch Surg. 1925; 10: 1-2.
6. Scott RB. Malignant changes in endometriosis. Obstet Gynecol. 1953; 2: 283-289.
7. Chu CN, Chen SW, Bai LY, Mou CH, Hsu CY, Sung FC. Increase in stroke mrisk in patients with head and neck cancer: a retrospective cohort study. Br J Cancer. 2011; 105: 1419-1423.
8. el-Newihi HM, Antaki JP, Rajan S, Reynolds TB. Large bloody ascites in association with pelvic endometriosis: case report and literature review. Am J Gastroenterol. 1995; 90: 632-634.
9. Naraynsingh V, Raju GC, Ratan P, Wong J. Massive ascites due to omental endometriosis. Postgrad Med J. 1985; 61: 539-540.
10. Stern RC, Dash R, Bentley RC, Snyder MJ, Haney AF, Robboy SJ. Malignancy in endometriosis: frequency and comparison of ovarian and extraovarian types. Int J Gynecol Pathol. 2001; 20: 133-139.
11. Dincer AD, Timmins P, Pietrocola D, Fisher H, Ambros RA. Primary peritoneal mullerian adenosarcoma with sarcomatous overgrowth associated with endometriosis: a case report. Int J Gynecol Pathol. 2002; 21: 65-68.
12. Raffaelli R, Piazzola E, Zanconato G, Fedele L. A rare case of extrauterine adenosarcoma arising in endometriosis of the rectovaginal septum. Fertil Steril. 2004; 81: 1142-1144.









































































































































{kind=link}