Neonatal Appendicitis
- 1. Paediatric Hospital of Coimbra Hospital Centre, University of Coimbra, Portugal
- 2. Maternity Bissaya Barreto Hospital Center, University of Coimbra, Portugal
Abstract
Acute appendicitis is a common disease in older children, but extremely rare in the neonate. Nevertheless, the true incidence might be underestimated, given the difficulty of the diagnosis. Subtle clinical signs and symptoms usually result in high morbidity and mortality due to delayed diagnosis and surgical intervention. The presentation of neonatal appendicitis can be identical to necrotizing enterocolitis, leading to misdiagnosis. Appendicitis should therefore be considered in the differential diagnosis for necrotizing enterocolitis and needs strong clinical suspicion.
We report a case of a premature newborn who presented with vomiting, abdominal distension and free intra-peritoneal air on plain x-ray. He was initially diagnosed and treated as necrotizing enterocolitis, but the absence of clinical improvement with standard treatment led to exploratory laparotomy. Surgical exploration revealed an acutely inflamed appendix with normal small and large intestines and appendectomy was performed. The post-operatory period was uneventful and the infant was discharged home. Follow-up confirmed a normal growth and neurodevelopment.
We herein report this case in order to raise awareness to this unusual pathology, so that an early diagnosis and treatment can lead to a better outcome, improving survival rate and reducing long term morbidity. We believe uncommon pathologies, like neonatal appendicitis, should be reported to facilitate proper epidemiologic studies.
Keywords
• Appendicitis
• Neonatal
• Necrotizing enterocolitis
• Chorioamnionitis
Citation
Gil AT, Morais S, Faria D (2014) Neonatal Appendicitis – an Uncommon Diagnosis, not to be Forgotten. JSM Clin Case Rep 2(4): 1048.
ABBREVIATIONS
NICU: Neonatal Intensive Care Unit; NEC: Necrotizing Enterocolitis
INTRODUCTION
Appendicitis in the neonatal period is rare, accounting for 0.1-0,2% of the appendicitis in infancy. However, the real incidence in the neonate is still uncertain [1]. It was first reported by Albrecht in 1905 in a one-month-old male infant who died of peritonitis [2].
The rarity of this pathology in this age group has been attributed to multiple factors, including the characteristic funnel, wide-opened shape of the appendix during the first 9-12 months of age (making blockage of the lumen less likely to occur), the liquid lacteous diet, the near-constant recumbent position of infants and the infrequent occurrence of infectious stimuli capable of inducing regional lymphatic hyperplasia [1, 3-7].
Some literature reports suggests that neonatal appendicitis is a different disease entity than the appendiceal inflammation and perforation that occurs later in life. Ischemia rather than obstruction seems to be the leading pathogenic factor, but the true etiology remains controverse, with some authors believing that neonatal appendicitis is nothing but an isolated form of NEC [4].
The clinical presentation is often subtle and non-specific, with anorexia, vomiting, diarrhea and abdominal distension being frequently reported. There are two main clinical presentations: the intra-abdominal (66-75%) and the intra-herniary forms (25- 33%) [1-2]. Intra-abdominal appendicitis is more likely mistaken for NEC, delaying the diagnosis and leading to a higher rate of perforation, peritonitis and a consequent higher mortality rate. Most cases of intra-herniary appendicitis, primarily associated with inguinal hernias, present with inguino-scrotal inflammatory signs, leading to an earlier diagnosis and a better outcome [1].
Suspicion for appendicitis should be made based on the clinical presentation and the results of laboratory and imagiologic tests, but often definitive diagnosis is made during surgical procedures or autopsy.
Main prognosis factor is the precocity of the diagnosis and surgical treatment, with appendectomy occurring before perforation as the ideal treatment [2]. The high perforation rate seen in neonatal appendicitis is usually attributed to a delay in diagnosis, a thin appendiceal wall and an indistensible cecum [7].
CASE PRESENTATION
A 2600g male was born at 36 weeks’ gestation to a twentyyear- old mother, mentally impaired, under psychiatric medication. All prenatal labs and ultra-sounds were normal. The neonate was born by vacuum assisted vaginal delivery and required resuscitation with positive pressure ventilation, with Apgar scores of 5, 8 and 9. Although there was a good recovery after birth, he maintained an expiratory grunt and supplementary oxygen requirements, so he was admitted to the Neonatal Intensive Care Unit (NICU) for surveillance and investigation.
At the time of admission to the NICU he had a normal physical examination, apart from tachypnea and intermittent expiratory grunt, and stable vital signs. He maintained need for supplementary oxygen (FiO2 25-28%) only in the first two hours of life. According to local protocols (prolonged time of membranes rupture (> 24H) and maternal fever), laboratory analysis was performed, which revealed a white blood cell count of 22,14 x 103/μL, a platelets count of 206 x 103/μL, a C-reactive protein level of 0,2 mg/dL and a procalcitonin level of 0,25 ng/mL. He was started on antibiotics (ampicillin and gentamicin). Blood culture taken on the first day of life did not grow any organisms.
A poor feeding tolerance was noted since day one of enteral feeding, with frequent episodes of gastro-esophageal reflux and occasional vomiting. On the 3th day of life he presented with jaundice, receiving phototherapy until the 7th day, with maximum bilirubin measurement of 340μmmol/L on day five.
On day four, the nasogastric tube started draining small amounts of gastric content prior to feeds and he started passing dark stools, guaiac-positive. On the seventh day of life, despite stable vital signs and no supplementary oxygen requirement, the clinical condition worsens, with lethargy, persistent vomiting and abundant bilious gastric drains. The abdomen was distended, with mild diffuse tenderness, without abdominal wall erythema or visible bowel loops. Laboratory studies found a C-reactive protein level of 4.3 mg/dL (rising from 2.1 mg/dL on day six), a white blood cell count of 26.51 x 103/μL and a platelets count of 363 x 103/μL. A plain abdominal x-ray in supine and lateral decubitus position showed diffusely dilated loops of bowel with air-fluid levels (Figure 1).
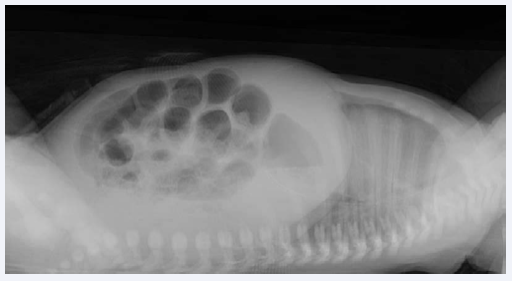
Figure 1 A plain abdominal x-ray taken in the seventh day of life showing diffusely dilated loops of bowel with air-fluid levels.
A presumptive diagnosis of intestinal obstruction associated with necrotizing enterocolitis was made and supportive treatment started. Previous antibiotics were stopped and vancomycin, ceftazidime and metronidazole were added.
Despite nasogastric tube decompression, cessation of feeding and antibiotics, on day nine of life, his condition was still not improving. Laboratory studies showed a C-reactive protein level of 16,9 mg/dL, a white blood cell count of 13,77 x 103/μL and a hypoalbuminemia of 29,8 g/L (normal values: 34 – 42g/L). Abdominal plain x-ray was repeated and revealed an image of free intra-peritoneal air (Figure 2).
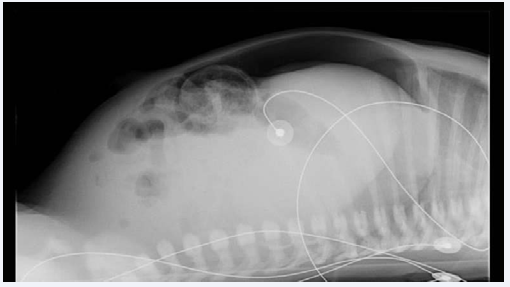
Figure 2 Abdominal plain x-ray repeated on day nine revealing an image of free intra-peritoneal air that lead to referral to a pediatric surgical center.
He was then transferred to a pediatric surgical center.
At exploratory laparotomy, an acutely inflamed appendix with a perforated tip and peritonitis were found. Small and large intestines were well perfused and there were no obvious signs of NEC, Hirschsprung’s disease or congenital anomalies of the gastrointestinal tract. Appendectomy was performed.
The surgical specimen sent for histological examination consisted of an appendix with 3.2 cm of length with a hemorrhagic distal tip. Histologic evaluation showed an exuberant acute inflammatory response, involving the serosa and sub-serosa layers, with a transmural process in some focal areas. An infiltrate of polymorphonuclear eosinophilic cells was seen and ganglion cells were normally present in the myenteric plexus. All these findings were consistent with a diagnosis of acute necrotizing appendicitis.
The post-operatory period was uneventful. Enteral feedings were started and advanced gradually. Blood culture during acute illness was negative. The infant achieved total enteral feedings four days after surgery and was discharged home 19 days after laparotomy, on day 28 of life.
He was seen in the outpatient clinic at 15 days, 1 month and 2 months after discharge, thriving well, with normal physical examination and spontaneous bowel movements. At 4 months a barium enema was performed that showed normal filling of the colon and terminal ileum. Last follow-up occurred at 20 months of age, with normal growth and neurodevelopment.
DISCUSSION
Neonatal appendicitis is a rare disease that occurs more commonly in male gender (male: female ratio of 3:1) and 25- 50% of all reported cases took place in premature infants [1,5,8]. The case reported herein is the first diagnosed case of neonatal appendicitis in our unit and it has occurred in a preterm male.
The etiology of neonatal appendicitis in the neonatal period remains unclear, but some authors suggest a strong association with NEC. Although histologically the two cannot be separated [8], there was no obvious evidence of NEC in our case: both small and large intestines were normal, inflammation was localized to the appendix and there was no pneumatosis in the plain x-ray. An extension of the proposal that ischemia is the main causal factor
in this age group [4], implicates conditions such as perinatal asphyxia, cardiac anomalies and other hypoxic states, as risk factors for neonatal appendicitis [8].On the other hand, common association with Hirschsprung’s disease or meconium ileus (frequent in cystic fibrosis) leads to the hypothesis that increased pressure at the appendiceal base may lead to inflammation and consequent perforation [9]. In this particular case there were no associated diseases and we can only speculate that there was a relative hypoxia at birth, because of the need for positive pressure ventilation in the first minutes of life.
We also cannot discard the role of maternal infection in the etiology of neonatal appendicitis, with at least two reports in the literature presenting cases of neonatal appendicitis associated with maternal chorioamnionitis [10-11]. In this case we do not have a definitive diagnosis of chorioamnionitis, since no amniotic fluid or placental cultures were performed, but we have some important clinical signs. The preterm premature
rupture of membranes and the maternal fever were valued and the newborn started antibiotic treatment on day one. The fact that the mother received antibiotic treatment during labor might explain why there was no positive blood culture in the newborn. We can speculate that although the newborn infection wasn’t prevented by the initial antibiotic treatment, it did minimize the inflammatory process leading to focalized infection in the appendix and a favorable outcome.
The diagnosis of acute appendicitis in the neonatal period requires a high suspicion index and must be considered in the differential diagnosis of acute abdomen in this age group. An early diagnosis and a timely surgical intervention are essential in avoiding perforation that, in this age group, rapidly leads to peritonitis with important mortality and morbidity associated. In our case although appendectomy was performed after appendix perforation and there were signs of peritoneal inflammation, the post-operatory period was uneventful and the outcome favorable with rapid and complete recovery.
Neonatal appendicitis continues to be a diagnostic challenge but, in this era of improved neonatal care, this entity should not be forgotten in the differential diagnosis for a neonate with acute abdomen, as perinatal conditions associated with appendicitis, such as prematurity and survival after severe hypoxia or ischemia, are increasingly common.
The case herein reported, raises the question whether maternal infection could have a role in the pathophysiologic process of neonatal appendicitis and reminds clinicians that an early surgical intervention is essential in assuring a favorable outcome in an otherwise severe condition.
ACKNOWLEDGEMENTS
Ana Teresa Gil developed the idea for the article, collected clinical data, performed the literature search and wrote the article. Sofia Morais was involved in critical revision of the manuscript. Dolores Faria managed the patient and was involved in critical revision of manuscript. All the authors approved the final version.









































































































































{kind=link}