Pneumoperitoneum, or not, that is the question- A Clinical Image
- 1. Department of Internal Medicine, Saint Joseph Hospital, USA
Citation
Senussi MH, Senussi NH, Bhattacharyya A, Sanders W (2013) Pneumoperitoneum, or not, that is the question- A Clinical Image. JSM Clin Case Rep 1(1): 1009.
CLINICAL IMAGE
Chilaiditi’s sign is an incidental radiological finding that may be mistaken for pneumoperitoneum and in the presence of symptoms (known as Chilaiditi’s syndrome), may potentially lead to unwarranted surgical intervention. We report a case of Chilaiditi’s syndrome in a 55-year-old woman presenting with vague epigastric pain who was ultimately found to have evidence of coronary ischemia with subsequent revascularization leading to complete symptom resolution. A 55-year-old woman presented with a 1-day history of fatigue and vague abdominal discomfort. She reported the insidious onset of mild to moderate, non-radiating, throbbing, epigastric pain that began 3-days prior to admission. She denied any similar symptoms in the past. The pain was associated with several bouts of non-bloody emesis. She denied any abdominal distention. She also denied any recent consumption of alcohol or use of NSAIDs. Past medical history included methadone use and chronic constipation. Her medications included methadone 5 mg once daily. No previous surgical history. She is a former intravenous heroin drug abuser.
On examination, blood pressure was 170/80 mmHg, pulse 79/min, oral temperature 97.8°F (36.6°C), Respiratory Rate 20/ min, and SpO2 97% on ambient air. Abdominal examination revealed mild epigastric tenderness with no signs of guarding or rigidity. A complete blood count revealed WBC 5.3 X 103/mm3, hemoglobin 11.4 g/dl, platelets 234 X 103/mm3. A comprehensive metabolic panel was within normal limits. Further laboratory studies included troponin level <0.01 ng/dl, TSH 1.1 uIU/ml, blood alcohol level <10 mg/dl, serum amylase and lipase were both within normal limits. A 12-lead EKG showed normal sinus rhythm with no acute ST or T-wave changes.
An upright antero-posterior and lateral plain-film radiographs of the abdomen revealed a raised right hemidiaphragm with what appeared to be subdiaphragmatic air (Figure 1,2).
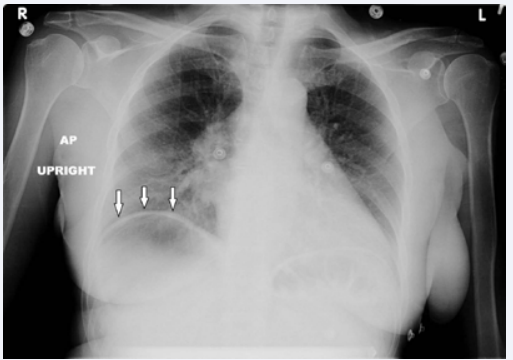
Figure 1 Upright abdominal radiograph revealing a raised right hemidiaphragm and a subdiaphragmatic lucency.
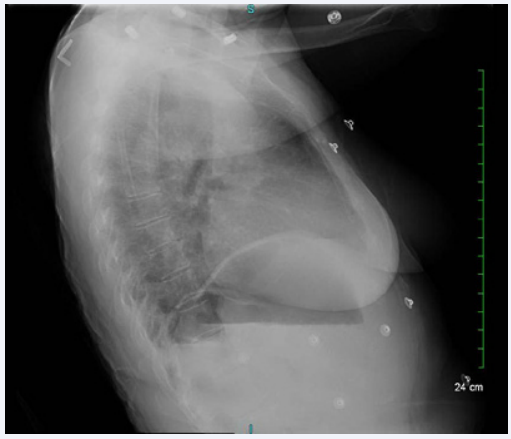
Figure 2 Upright abdominal radiograph revealing a raised right hemidiaphragm and a subdiaphragmatic lucency.
A computed tomographic scan of the abdomen confirmed the presence of a bowel loop interpositioned between the diaphragm and the right hepatic lobe with no evidence of free intra-peritoneal air (Figure 3).
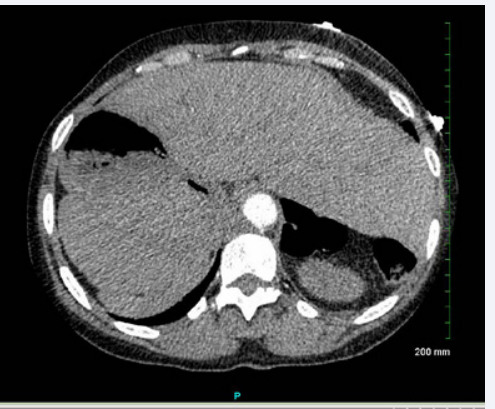
Figure 3 Non-contrast computed tomographic scan of abdomen confirming the presence of a bowel loop interpositioned between the right hepatic lobe and diaphragm with no evidence of free peritoneal air.
This was identified as Chilaiditi’s sign, an illusion of free air due to the presence of a gas-filled transverse colon positioned between the right hemi-diaphragm and the liver. The patient was found have increasing troponins and evidence of ischemia on 12- Lead EKG. The patient underwent percutaneous revascularization with stent placement for a 90% stenosis of the mid-right coronary artery, leading to complete symptom resolution.
DISCUSSION
Chilaiditi’s sign is an incidental radiological finding with a prevalance rate of approximately 0.1 to 0.25% of all chest radiographs [1]. It is characterized by the asymptomatic hepatodiaphragmatic interposition of the colon leading to an illusion of air under the diaphragm. Contributing factors include advanced age, male gender, pregnancy, chronic lung disease, cirrhosis, ascites, chronic constipation, bed-ridden state, aerophagia, and absence of suspensory ligaments of the transverse colon or falciform ligament [1]. Chilaiditi’s syndrome may be associated with nausea, vomiting, abdominal pain, constipation or anorexia and may be mistaken for pneumoperitoneum. The identification of a haustral pattern of the subdiaphragmatic lucency is helpful in identifying this radiological sign but may require further imaging with a CT scan [2].
CONCLUSIONS
Chilaiditi’s sign, although rare, should be considered when reading chest radiographs. In the presence of symptoms this may be mistaken for pneumoperitoneum and lead to unnecessary surgical intervention. The presence of haustral patterns and plicae circularis is helpful in identifying this sign and may require further imaging with a computed tomographic scan.









































































































































{kind=link}